Laparoscopic Cystectomy Coding
Jonathan Rubenstein, MD
Chesapeake Urology Associates, Baltimore, MD
[Rev Urol. 2016;18(3):157-158 doi: 10.3909/riu0728]
© 2016 MedReviews®, LLC
Laparoscopic Cystectomy Coding
Jonathan Rubenstein, MD
Chesapeake Urology Associates, Baltimore, MD
[Rev Urol. 2016;18(3):157-158 doi: 10.3909/riu0728]
© 2016 MedReviews®, LLC
Laparoscopic Cystectomy Coding
Jonathan Rubenstein, MD
Chesapeake Urology Associates, Baltimore, MD
[Rev Urol. 2016;18(3):157-158 doi: 10.3909/riu0728]
© 2016 MedReviews®, LLC
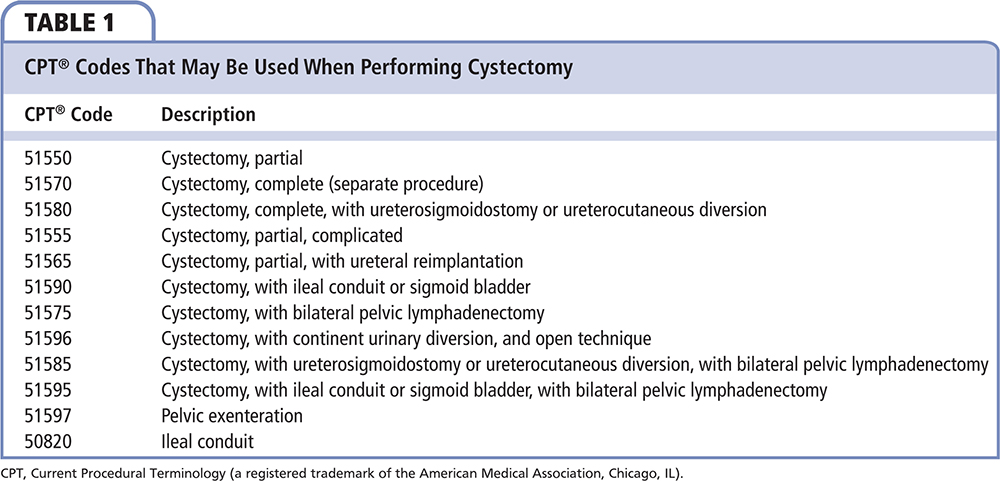
Although the open (incisional) approach to cystectomy (simple or radical) is regarded as a standard approach to the surgical removal of the bladder for benign and malignant conditions, laparoscopic and robot-assisted approaches are becoming more popular. Laparoscopic and robotic cystectomy procedures can be safely performed with acceptably low risk of blood loss, transfusion, and intraoperative complications.1,2 However, because no specific Current Procedural Terminology (CPT® [American Medical Association, Chicago, IL]) codes exist for the performance of these procedures, and due to the significantly varied procedures (eg, completing the procedure only partially or completely laparoscopic or robotic, whether it is for cancer or benign conditions, the type of urinary diversion that is performed, whether a lymph node dissection is performed, if a prostatectomy or hysterectomy is also performed, and so on), choosing the correct CPT code to submit has been a matter of debate. Codes that are often used for cystectomy procedures are listed in Table 1.
Traditional teaching for coding laparoscopic procedures is to choose the laparoscopic code when the procedure is performed laparoscopically, and the open code when it is performed using an incisional technique. CPT codes typically have a vignette that describes the basics of the procedure and typical work that is included in the procedure as a basis for valuing the code. For example, when choosing CPT codes for nephrectomy, CPT 50545 should be chosen for laparoscopic radical nephrectomy and CPT 50230 for open radical nephrectomy (or CPT 50225 if the nephrectomy is complicated due to prior surgery in the area). For simple nephrectomy (noncancerous conditions), the codes are CPT 50546 and CPT 50220 for the laparoscopic and open procedures, respectively.
However, this is not as simple when approaching cystectomy. We are taught that an unlisted procedure code should be used when no specific CPT code exists for the procedure being performed. When submitting for reimbursement, we are taught to choose a procedure with comparable work as a reference for reimbursement. In the case of cystectomy, the code to submit is CPT 51999 Unlisted laparoscopic procedure bladder, and the work submitted should be compared with the open cystectomy code. Because CPT 51999 is an unspecified code, other components of the procedure are not bundled or described; therefore, CPT codes for other aspects of the procedure that are performed, with their corresponding work, should also be submitted. For example, CPT 55866 for laparoscopic prostatectomy, CPT 58543 and CPT 58541 for laparoscopic hysterectomy (> 250 g or < 250 g, respectively), CPT 38771 and CPT 38772 for laparoscopic pelvic lymph node dissection (without or with periaortic sampling, respectively), and CPT 50820 for ileal conduit should be billed when performed due to the work involved in performing those procedures. In some cases, a prearranged contract with the insurer for the procedure can be negotiated. Recently, we have learned that some insurers have stopped reimbursing a fair value for the work involved when performing procedures and using unlisted codes, such as CPT 51999, but instead are choosing a reimbursement level much below that of the work that was actually performed. Due to the significant work involved and expertise needed when performing these procedures, a fair value for reimbursement is important.
When looking deeper into the cystectomy codes themselves, unlike the nephrectomy codes in which there is a laparoscopic and open code with corresponding vignettes, we see that no vignette exists for cystectomy, and no approach (open or laparoscopic) is specifically described. That means that the same cystectomy codes that describe bladder removal and associated procedures can be used no matter what the approach (open, laparoscopic, or robotic). So which CPT codes should be chosen and submitted? Sadly, as some insurers have turned patient care into a cat-and-mouse game, code choice may be based upon individual insurer contracts. If the insurer is allowing a fair reimbursement for using an unlisted code when performing a laparoscopic cystectomy, then the unlisted code may be chosen. However, if the insurer is paying well below fair reimbursement, then it is not wrong to use typical cystectomy codes when submitting for reimbursement. ![]()
References
- Novara G, Catto JW, Wilton T, et al. Systematic review and cumulative analysis of perioperative outcomes and complications after robot-assisted radical cystectomy. Eur Urol. 2015;67:376-401.
- Deboudt C, Perrouin-Verbe MA, Le Normand L, et al. Comparison of the morbidity and mortality of cystectomy and ileal conduit urinary diversion for neurogenic lower urinary tract dysfunction according to the approach: laparotomy, laparoscopy or robotic [published online July 17, 2016]. Int J Urol. doi: 10.1111/iju.13166.