Management of Erectile Dysfunction in the Hypogonadal Man: A Case-Based Review
Ranjith Ramasamy, MD, Jason M. Scovell, BBA, Nathan A. Wilken, BS, Jason R. Kovac, MD, Larry I. Lipshultz, MD
Scott Department of Urology, Baylor College of Medicine, Houston, TX
Erectile dysfunction (ED) has emerged as an important marker of cardiovascular and overall health, independent of other known conventional risk factors. ED often precedes coronary artery disease in half of affected subjects, and could indicate the presence of cardiovascular pathology. The pathophysiology and role of androgens in sexual function are described, along with the relevant literature on the effects of aging in erectile and gonadal function. The concept of testosterone supplementation (TST) in men with ED is reviewed. The authors utilize clinical vignettes to discuss the appropriate management of two clinical cases of men at different life stages who have ED in the setting of hypogonadism and propose a treatment algorithm. In patients of all ages, proper identification of the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, phosphodiesterase type 5 inhibitors, or both, in the management of these disorders.
[Rev Urol. 2014;16(3):105-109 doi: 10.3909/riu0623]
© 2014 MedReviews®, LLC
Management of Erectile Dysfunction in the Hypogonadal Man: A Case-Based Review
Ranjith Ramasamy, MD, Jason M. Scovell, BBA, Nathan A. Wilken, BS, Jason R. Kovac, MD, Larry I. Lipshultz, MD
Scott Department of Urology, Baylor College of Medicine, Houston, TX
Erectile dysfunction (ED) has emerged as an important marker of cardiovascular and overall health, independent of other known conventional risk factors. ED often precedes coronary artery disease in half of affected subjects, and could indicate the presence of cardiovascular pathology. The pathophysiology and role of androgens in sexual function are described, along with the relevant literature on the effects of aging in erectile and gonadal function. The concept of testosterone supplementation (TST) in men with ED is reviewed. The authors utilize clinical vignettes to discuss the appropriate management of two clinical cases of men at different life stages who have ED in the setting of hypogonadism and propose a treatment algorithm. In patients of all ages, proper identification of the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, phosphodiesterase type 5 inhibitors, or both, in the management of these disorders.
[Rev Urol. 2014;16(3):105-109 doi: 10.3909/riu0623]
© 2014 MedReviews®, LLC
Management of Erectile Dysfunction in the Hypogonadal Man: A Case-Based Review
Ranjith Ramasamy, MD, Jason M. Scovell, BBA, Nathan A. Wilken, BS, Jason R. Kovac, MD, Larry I. Lipshultz, MD
Scott Department of Urology, Baylor College of Medicine, Houston, TX
Erectile dysfunction (ED) has emerged as an important marker of cardiovascular and overall health, independent of other known conventional risk factors. ED often precedes coronary artery disease in half of affected subjects, and could indicate the presence of cardiovascular pathology. The pathophysiology and role of androgens in sexual function are described, along with the relevant literature on the effects of aging in erectile and gonadal function. The concept of testosterone supplementation (TST) in men with ED is reviewed. The authors utilize clinical vignettes to discuss the appropriate management of two clinical cases of men at different life stages who have ED in the setting of hypogonadism and propose a treatment algorithm. In patients of all ages, proper identification of the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, phosphodiesterase type 5 inhibitors, or both, in the management of these disorders.
[Rev Urol. 2014;16(3):105-109 doi: 10.3909/riu0623]
© 2014 MedReviews®, LLC
Key words
Erectile dysfunction • Testosterone supplementation • Hypogonadism • Phosphodiesterase type 5 inhibitors
Key words
Interstitial cystitis • Bladder pain syndrome • Chronic disease • Autoimmune diseases
In light of the recent evidence associating testosterone with cardiovascular risk in elderly men, testosterone supplementation therapy should be used judiciously in the management of ED in older men.
Testosterone therapy alone appears to be beneficial for improvement in sexual function, but not when used in combination with PDE5i.
Main Points
• Phosphodiesterase-5 inhibitors (PDE5i) and testosterone supplementation therapy (TST) are established treatment strategies for erectile dysfunction (ED) and hypogonadism, respectively.
• Testosterone has been shown to affect multiple neurologic and vascular points of the erectile pathway and acts on signaling pathways in the hypothalamus and amygdale, which is important considering that the central nervous system modulates sexual desire and libido.
• With the progressive increase in the proportion of elderly men, an interest in characterizing the prevalence of ED and hypogonadism has developed. TST alone appears to be beneficial for improvement in sexual function, but not when used in combination with PDE5i.
• In the case of a younger, otherwise healthy patient, TST alone should be considered, as his ED would most likely be classified as having a psychogenic component.
• Taken together, therapy with a PDE5i is the more prudent first-line approach to the overall clinical scenario in an elderly man with ED. Identifying the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, PDE5i, or both, in the management of these disorders.
Main Points
• Phosphodiesterase-5 inhibitors (PDE5i) and testosterone supplementation therapy (TST) are established treatment strategies for erectile dysfunction (ED) and hypogonadism, respectively.
• Testosterone has been shown to affect multiple neurologic and vascular points of the erectile pathway and acts on signaling pathways in the hypothalamus and amygdale, which is important considering that the central nervous system modulates sexual desire and libido.
• With the progressive increase in the proportion of elderly men, an interest in characterizing the prevalence of ED and hypogonadism has developed. TST alone appears to be beneficial for improvement in sexual function, but not when used in combination with PDE5i.
• In the case of a younger, otherwise healthy patient, TST alone should be considered, as his ED would most likely be classified as having a psychogenic component.
• Taken together, therapy with a PDE5i is the more prudent first-line approach to the overall clinical scenario in an elderly man with ED. Identifying the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, PDE5i, or both, in the management of these disorders.
Erectile dysfunction (ED) has emerged as an important marker of cardiovascular and overall health, independent of other known conventional risk factors. Because ED often precedes coronary artery disease (CAD) in half of affected subjects, it may be considered a harbinger of indolent cardiovascular pathology.1,2 The modulation of erectile function by testosterone is well known,3,4
and in men with both hypogonadism and ED a treatment strategy necessitating management of both conditions is required.
Phosphodiesterase type 5 inhibitors (PDE5i) and testosterone supplementation therapy (TST) are established treatment strategies for ED and hypogonadism, respectively. Using a PDE5i in combination with TST has the potential for improving efficacy in men with concurrent ED and hypogonadism compared with the use of either agent alone. However, in light of the recent evidence associating testosterone with cardiovascular risk in elderly men,5,6 TST should be used judiciously in the management of ED in older men.
The Role of Androgens in Sexual Function
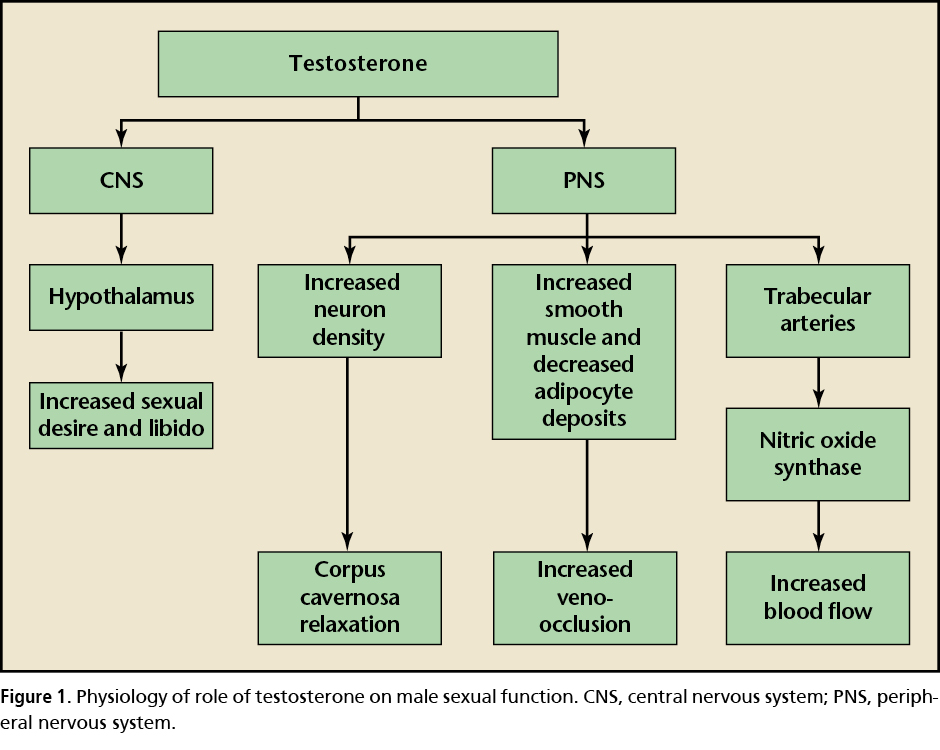
An erection is the result of parasympathetic signaling in response to activation of reflexogenic and psychogenic signals that ultimately lead to engorgement of the penis. The erectile pathway starts with acetycholine efflux from nerve terminals in the penis causing nitric oxide (NO) release from arterial endothelial cells leading to vasodilation and increased blood flow.7 This increased volume of blood within the vascular bed of the corpus cavernosum leads to compression of penile venules, resulting in veno-occlusion and tumescence. Detumescence is subsequently achieved via cyclic guanosine monophosphate (GMP) degradation and activation of the PDE5 enzyme, resulting in smooth muscle contraction.7
Testosterone has been shown to affect multiple points of the erectile pathway: the central nervous system, the postganglionic sympathetic neurons in the penis, and the penile trabecular arteries (Figure 1). Furthermore, testosterone acts on signaling pathways in the hypothalamus and amygdale,8 which is important considering that the central nervous system modulates sexual desire and libido.9 Peripherally, testosterone increases nonadrenergic noncholinergic neuron density, leading to increased relaxation of the corpus cavernosum.3 Within the endothelial cells of the trabecular arteries, testosterone leads to an increase in NO synthase activity followed by increased NO levels and smooth muscle relaxation. Decreased testosterone also affects the subtunical architecture, leading to decreased smooth muscle, via apoptosis, and increased adipocyte deposits in the corpora cavernosa.10,11 Both of these alterations lead to decreased veno-occlusion, thereby increasing propensity for venous leaks. Testosterone appears to play an important role in regulating sexual function.
Effect of Aging on Erectile and Gonadal Function
With the progressive increase in the proportion of elderly men, an interest in characterizing the prevalence of ED and hypogonadism has developed. Data from the Massachusetts Male Aging Study, a community-based, random sample observational survey of men aged 40 to 70 years (N = 774), found that the prevalence of complete ED increased from 5% to 15% as patients aged from 40 to 70 years.12 As expected, the rate of ED was substantially higher among men with comorbidities, such as type 2 diabetes (26%) and cardiovascular disease (58.3%), compared with the general population (10%). In another large (N = 31,742) cross-sectional analysis of male health professionals between the ages of 50 and 90 years, investigators noted an inverse relationship between age and sexual function (ie, increased age leads to decreased sexual function).13 Furthermore, only 2% of men reported ED before the age of 40, with the prevalence increasing to 26% in men 50 to 59 years old, and to 40% in men 60 to 69 years old.13
Defining the prevalence of hypogonadism in the general population is difficult due to the debate surrounding the definition of the condition. The Hypogonadism in Males (HIM) study estimated the prevalence of hypogonadism (total testosterone < 300 ng/dL) in men aged ≥ 45 years to be 39%.14 The cutoff level of testosterone for diagnosis of hypogonadism ranges from < 202 to < 404 ng/dL, and based on these numbers the prevalence of hypogonadism in men with ED varies from 7% to 47%.15 Given that testosterone levels decrease, and vascular compromise occurs with age, elderly men are more likely to be concurrently diagnosed with ED and hypogonadism.
Role of Testosterone Therapy in ED
Testosterone is known to correlate with both libido and erectile function. In the European Male Aging Study (EMAS), men between the ages of 40 and 79 years (N = 3369) showed a correlation between low serum testosterone and sexual function.16 Men with normal serum testosterone levels were less likely to have decreased frequency of morning erections, decreased erectile function, and decreased frequency of sexual thoughts.16 In a study of TST with gels or patches (N = 227), hypogonadal men reported improvements in sexual motivation, desire, and enjoyment with a partner, and increased overall sexual performance score.17 There was also an increase in percentage of men reporting full erections and greater satisfaction with erections. These benefits were maximally achieved within the first 30 days after initiation of TST and remained constant over the course of the study.17 In a recent study by Finkelstein and colleagues,18 healthy men between the ages of 20 and 50 years (N = 400) were chemically castrated with goserelin. Men who received testosterone replacement had improvements in both sexual desire and erectile function.
Animal studies have also demonstrated the relationship between testosterone and erectile function. Mills and colleagues19 showed that decreased cavernosal pressure in castrated rats was restored with testosterone replacement, suggesting a critical role for testosterone in the maintenance of penile vascular smooth muscle responsiveness. These findings were then corroborated by another study that also demonstrated the ability of testosterone to restore erectile function in castrated rats.20
When used alongside a PDE5i in men with ED, TST has not been shown to yield any additional benefits. In a randomized study by Spitzer and colleagues,21 the authors found no improvement in erectile function when they compared sildenafil (PDE5i) alone versus sildenafil in combination with TST in patients with ED and low testosterone.21 Unfortunately, the efficacy of testosterone alone in treating ED was not assessed in this population. As such, testosterone therapy alone appears to be beneficial for improvement in sexual function, but not when used in combination with PDE5i.
Algorithm for Management of ED in Hypogonadal Male
Case 1
Mr. A, age 33, presented with low libido and ED that had been worsening over the past several months. Mr. A had no other medical history, and his physical examination demonstrated bilaterally descended testes (∼16 mL) and a circumcised penis with no evidence of Peyronie’s plaques. Serum total testosterone (× 2 in the morning) was ∼250 ng/dL (normal, 300-800 ng/dL).
Case 2
Mr. B, age 73, presented with low libido and ED that had been worsening over the past several years. Mr. B also has CAD, non–insulin-dependent diabetes, hypertension, history of cerebrovascular accident (CVA), and dyslipidemia with normal renal and pulmonary function. His physical examination demonstrated bilaterally descended testes (∼16 mL) and a circumcised penis with no evidence of Peyronie’s plaques. His serum total testosterone (× 2 in the morning) was ∼250ng/dL.
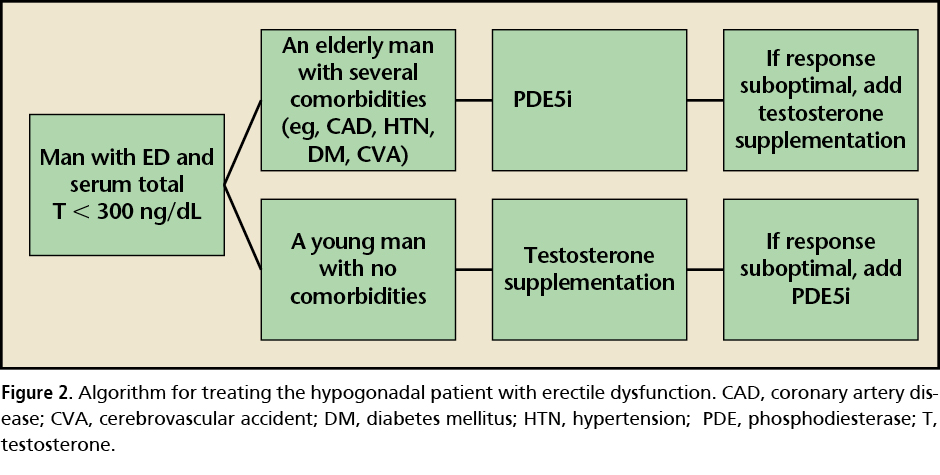
These two patients highlight common clinical problems that require different approaches to management (Figure 2). The practitioner must consider the risks and benefits of TST for low libido and ED in the hypogonadal man based on the data regarding efficacy and potential adverse effects. The issue of whether to use PDE5i and TST in combination or sequentially has been controversial.3,22
Based on the literature, a different management approach to these two patients can be advocated. In the younger, otherwise healthy patient (Mr. A), TST alone should be considered. Mr. A’s ED would most likely be classified as having a psychogenic component. Mr. A needs to be investigated for symptoms of hypogonadism, such as decreased libido, lack of energy, and fatigue. If symptoms of hypogonadism were present, along with low serum testosterone, he would benefit from treatment with TST. Because this patient is young, adequate counseling about the loss of fertility and testicular atrophy needs to be stressed. When desired, testosterone could be used in combination with intramuscular human chorionic gonadotropin to preserve fertility and testicular volume.23
In contrast, the management for the elderly man with comorbidities such as CAD and a prior CVA (Mr. B) presents a more complicated clinical scenario. His ED is most likely organic, and is unlikely to benefit from TST alone. In light of the recent controversial evidence, the cardiovascular risk factors in this patient should bring the clinician’s attention to the putative association between TST and increased cardiovascular adverse events in the elderly comorbid population.5,6,24 Low libido in this elderly man should remain a paramount concern to the practitioner. Interestingly, PDE5i alone can increase endogenous serum testosterone in hypogonadal men21 and can potentially improve the libido. In addition, recent studies have shown several pleiotropic beneficial effects of PDE5i in patients with CAD, hypertension, heart failure, pulmonary arterial hypertension, or diabetes mellitus.25
Taken together, we believe that a PDE5i is the more prudent first-line approach to the overall clinical scenario in this elderly man with ED. Proper identification of the underlying pathophysiology of decreased libido and erectile function is paramount in choosing between the use of TST, PDE5i, or both, in the management of these disorders. ![]()
Ranjith Ramasamy, Jason M. Scovell, Nathan A. Wilken, and Jason R. Kovac have no conflicts of interest to report. Larry I. Lipshultz is a clinical trials participant, consultant, and speaker for Auxilium Pharmaceuticals and Endo Health Solutions.
References
- Thompson IM, Tangen CM, Goodman PJ, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005; 294:2996-3002.
- Miner MM. Erectile dysfunction: a harbinger for cardiovascular events and other comorbidities, thereby allowing a ‘Window of Curability’. Int J Clin Pract. 2009;63:1123-1126.
- Isidori AM, Buvat J, Corona G, et al. A critical analysis of the role of testosterone in erectile function: from pathophysiology to treatment-a systematic review. Eur Urol. 2014;65:99-112.
- Castela A, Vendeira P, Costa C. Testosterone, endothelial health, and erectile function. ISRN Endocrinol. 2011;2011:839149.
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of non-fatal myocardial infarction following testosterone therapy prescription in men. PLoS One. 2014;9:e85805.
- Vigen R, O’Donnell CI, Baron AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829-1836.
- McVary KT. Clinical practice. Erectile dysfunction. N Engl J Med. 2007;357:2472-2481.
- Angelbeck JH, DuBrul EF. The effect of neonatal testosterone on specific male and female patterns of phosphorylated cytosolic proteins in the rat preoptic-hypothalamus, cortex and amygdala. Brain Res. 1983;264:277-283.
- Hull EM, Lorrain DS, Du J, et al. Hormone-neurotransmitter interactions in the control of sexual behavior. Behav Brain Res. 1999;105:105-116.
- Traish A, Kim N. The physiological role of androgens in penile erection: regulation of corpus cavernosum structure and function. J Sex Med. 2005;2: 759-770.
- 11.Traish AM, Toselli P, Jeong SJ, Kim NM. Adipocyte accumulation in penile corpus cavernosum of the orchiectomized rabbit: a potential mechanism for veno-occlusive dysfunction in androgen deficiency. J Androl. 2005;26:242-248.
- Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151:54-61.
- Bacon CG, Mittleman MA, Kawachi I, et al. Sexual function in men older than 50 years of age: results from the health professionals follow-up study. Ann Intern Med. 2003;139:161-168.
- Mulligan T, Frick MF, Zuraw QC, et al. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract. 2006;60:762-769.
- Köhler TS, Kim J, Feia K, et al. Prevalence of androgen deficiency in men with erectile dysfunction. Urology. 2008;71:693-697.
- Wu FC, Tajar A, Beynon JM, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363:123-135.
- Wang C, Swerdloff RS, Iranmanesh A, et al. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. J Clin Endocrinol Metab. 2000;85:2839-2853.
- Finkelstein JS, Lee H, Burnett-Bowie SA, et al. Gonadal steroids and body composition, strength, and sexual function in men. N Engl J Med. 2013;369:1011-1022.
- Mills TM, Wiedmeier VT, Stopper VS. Androgen maintenance of erectile function in the rat penis. Biol Reprod. 1992;46:342-348.
- Giuliano F, Rampin O, Schirar A, et al. Autonomic control of penile erection: modulation by testosterone in the rat. J Neuroendocrinol. 1993;5:677-683.
- Spitzer M, Basaria S, Travison TG, et al. Effect of testosterone replacement on response to sildenafil citrate in men with erectile dysfunction: a parallel, randomized trial. Ann Intern Med. 2012;157:681 691.
- Jannini EA, Isidori AM, Aversa A, et al. Which is first? The controversial issue of precedence in the treatment of male sexual dysfunctions. J Sex Med. 2013;10: 2359-2369.
- Hsieh TC, Pastuszak AW, Hwang K, Lipshultz LI. Concomitant intramuscular human chorionic gonadotropin preserves spermatogenesis in men undergoing testosterone replacement therapy. J Urol. 2013;189:647-650.
- Basaria S, Coviello AD, Travison TG, et al. Adverse events associated with testosterone administration. N Engl J Med. 2010;363:109-122.
- Chrysant SG. Effectiveness and safety of phosphodiesterase 5 inhibitors in patients with cardiovascular disease and hypertension. Curr Hypertens Rep. 2013;15:475-483.