Alexander Guminski, MD, PhD1; Christopher M. Pieczonka, MD2; Bryan A. Mehlhaff, MD3; Antonio Fojo, MD4; Anthony M. Joshua, MD, PhD5,6
1Department of Medical Oncology, Royal North Shore Hospital, Northern Clinical School, University of Sydney, St Leonards, New South Wales, Australia
2Associated Medical Professionals, Syracuse, New York, USA
3Oregon Urology Institute, Springfield, USA
4Department of Medical Oncology, NewYork-Presbyterian/Columbia University Medical Center, New York, USA
5Department of Medical Oncology, Kinghorn Cancer Centre, St Vincent’s Hospital, Darlinghurst, New South Wales, Australia
6School of Clinical Medicine, University of New South Wales Medicine and Health, Sydney, New South Wales, Australia
KEYWORDS:
Abiraterone acetate; biological availability; neoplasm metastasis; pharmacokinetics; prostatic neoplasms
Abstract
Background: Prostate cancer is the second-most common malignancy and fourth-leading cause of cancer mortality in men worldwide, and the incidence of metastatic castration-resistant prostate cancer (mCRPC) has increased in recent years. The selective, irreversible cytochrome P450 17α-hydroxylase/C17, 20-lyase inhibitor abiraterone has demonstrated efficacy and safety in patients with mCRPC, with US Food and Drug Administration approval granted to originator abiraterone acetate (OAA) for mCRPC in 2011 and metastatic castration-sensitive prostate cancer in 2018. Because of the poor solubility, pharmacokinetic parameters, and demonstrated food effect of OAA, the abiraterone acetate fine particle (AAFP) formulation was developed and received Food and Drug Administration approval for mCRPC in 2018 based on clinical results demonstrating bioequivalence to OAA.
Methods: We performed a literature search on the National Library of Medicine’s PubMed database across all time points for studies assessing the food effect and pharmacokinetic parameters of abiraterone formulations. We then summarized the food effect for both OAA and AAFP formulations, with a focus on treatment exposure and other pharmacokinetic parameters. We also assessed implications for tolerability and safety based on the relative bioavailability of abiraterone.
Results: Clinical studies from our search showed that although AAFP formulation has also demonstrated a food effect for fed vs fasted administration, this effect is decreased compared with OAA. Abiraterone acetate fine particle formulation can be administered with or without food, whereas OAA must be administered in a modified fasting state.
Conclusion: The available data suggest a potentially improved risk-benefit ratio for AAFP formulation compared with OAA.
Prostate cancer is the second-most common malignancy in men worldwide, behind only lung cancer, with an age-standardized incidence of 29.4 per 100 000 individuals and an age-standardized mortality rate of 7.3 per 100 000 individuals reported in 2022.1 The incidence of metastatic prostate cancer has increased in recent years, particularly in men aged 55 to 69 years.2 Androgen-deprivation therapy (ADT) is recommended in combination with an androgen receptor pathway inhibitor with or without docetaxel as initial therapy to treat metastatic hormone-naive or castration-sensitive prostate cancer and is highly effective in this population.3,4 Resistance to ADT can develop, however, leading to progression to the lethal phenotype of metastatic castration-resistant prostate cancer (mCRPC).
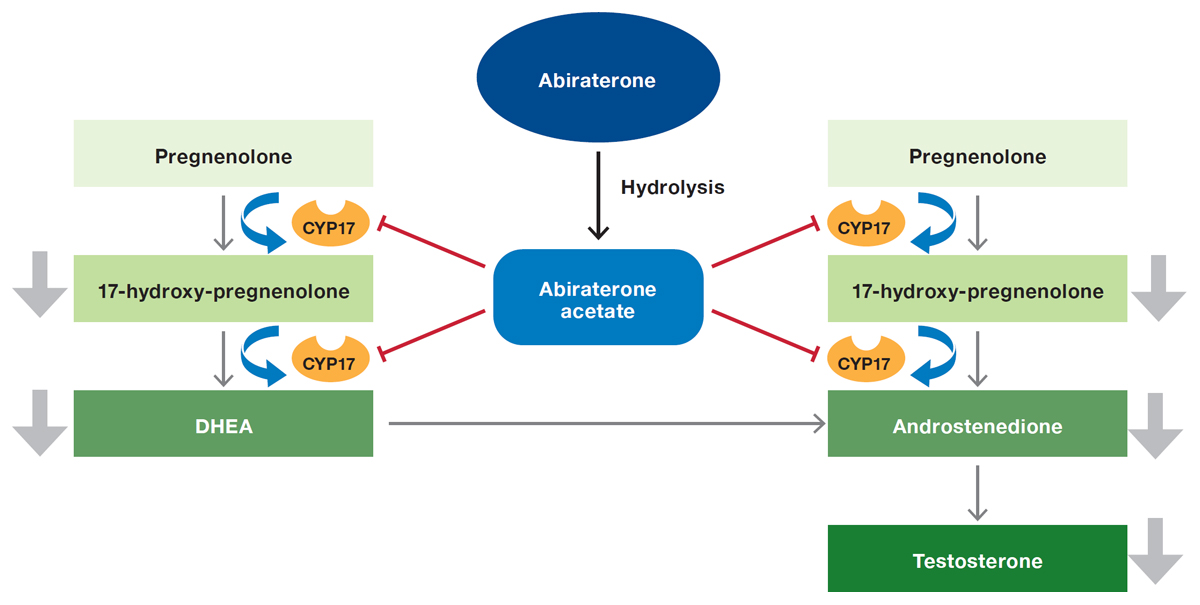
Abiraterone is a selective, irreversible inhibitor of cytochrome P450 17α-hydroxylase/C17, 20-lyase (CYP17), a key enzyme involved in androgen synthesis (Figure 1). A series of phase 3 trials of originator abiraterone acetate (OAA; Zytiga [Janssen Biotech, Inc]), a prodrug formulation of abiraterone, demonstrated efficacy and safety in patients with mCRPC, previously treated with docetaxel or not, as well as patients with metastatic castration-sensitive prostate cancer.5,6 Based on these pivotal studies, OAA 1000 mg in combination with prednisone 5 mg once daily was approved by the US Food and Drug Administration for the treatment of patients with mCRPC in 2011 and for patients with metastatic castration-sensitive prostate cancer in 2018.7 The addition of low-dose prednisone to OAA therapy prevents mineralocorticoid excess resulting from inhibition of CYP17A1, reducing the incidence and severity of associated adverse events (AEs) such as hypokalemia, hypertension, and fluid retention.8 Originator abiraterone acetate is classified as a class IV compound by the biopharmaceutical classification system, indicating that it has low oral bioavailability and poor water solubility and exhibits large variability in exposure in healthy individuals9; class IV compounds also generally have large interpatient and intrapatient variability regarding absorption. As would be expected given this classification, various trials have demonstrated high levels of variability in exposure (eg, area under the concentration-time curve and observed maximum serum concentration [Cmax ]) for OAA in healthy participants and patients with mCRPC.9,10 A substantial food effect is also associated with OAA, which further exacerbates the observed variability in its levels.
The abiraterone acetate fine particle (AAFP; Yonsa [Sun Pharmaceutical Industries, Inc]) formulation was developed using SoluMatrix Fine Particle Technology (iCeutica, Inc) to increase bioavailability and to mitigate the high pharmacokinetic variability and food effects often exhibited by lipophilic, poorly water-soluble pharmaceutical agents.11 The STAAR study (ClinicalTrials.gov identifier NCT02737332) reported bioequivalence and therapeutic equivalence between AAFP 500 mg daily and OAA 1000 mg daily,12 with no impact on efficacy or safety reported in patients who switched from OAA to AAFP in the STAAR study extension.13 Based on these studies and existing evidence for OAA, AAFP was approved in 2018 by the Food and Drug Administration for the treatment of patients with mCRPC in combination with methylprednisolone; the National Comprehensive Cancer Network also recommends OAA or AAFP plus corticosteroids for the treatment of patients with mCRPC.3,13
Figure 1. The mechanism of action of abiraterone acetateAbbreviations: CYP17, cytochrome P450 17α-hydroxylase/C17, 20-lyase; DHEA, dehydroepiandrosterone.
This article provides an overview of the food effect observed for OAA and AAFP in healthy participants and patients with prostate cancer, with a focus on treatment exposure and other pharmacokinetic parameters, as well as a discussion of the implications for tolerability and safety of the relative bioavailability of OAA and AAFP. Various strategies to manage the food effect associated with abiraterone are also briefly summarized, including concomitant administration of abiraterone acetate and food, therapeutic monitoring approaches, and modified formulations of the drug.
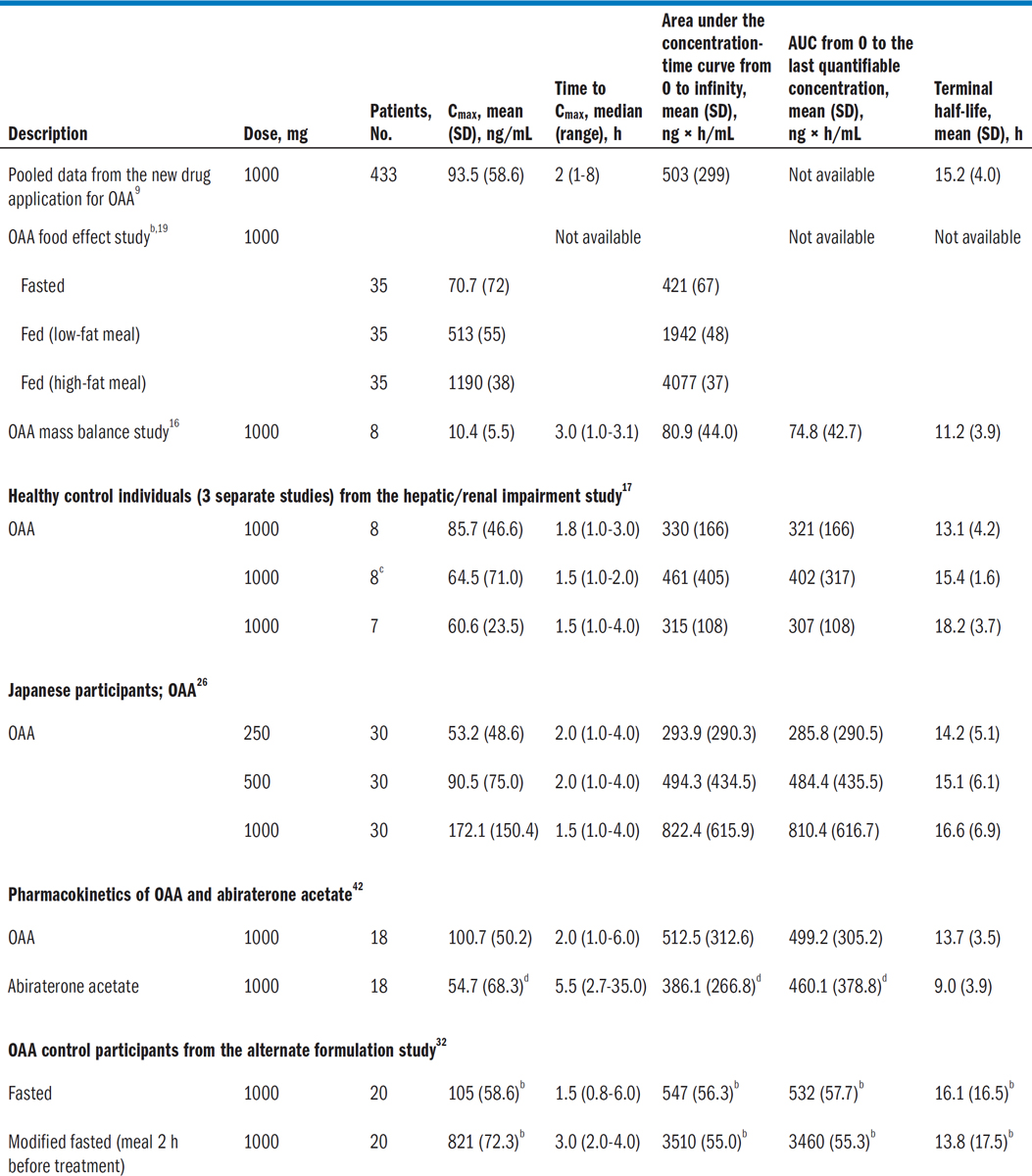
Abiraterone acetate is an inactive prodrug that is quickly converted to abiraterone, the parent compound and main metabolite of abiraterone acetate; most pharmacokinetic studies have focused on abiraterone, considering that the acetate form is hydrolyzed quickly in intestinal fluids.14 Although pharmacokinetic parameters are reported for abiraterone acetate, the prodrug was not detected in any pharmacokinetic samples in a phase 1 study of OAA, indicating rapid conversion to the parental compound.15 In a fasted state, absorption of abiraterone is rapid, with the Cmax generally occurring within 2 hours and ranging from 100 ng/mL to 300 ng/mL and with the area under the concentration-time curve ranging from 600 to 1500 ng × h/mL.14,16,17 Abiraterone absorption is also complex, with the key factors affecting exposure in a pharmacokinetic model for a population with mCRPC being health status (healthy participants vs participants with mCRPC) and concomitant food intake (fed vs fasted).18,19
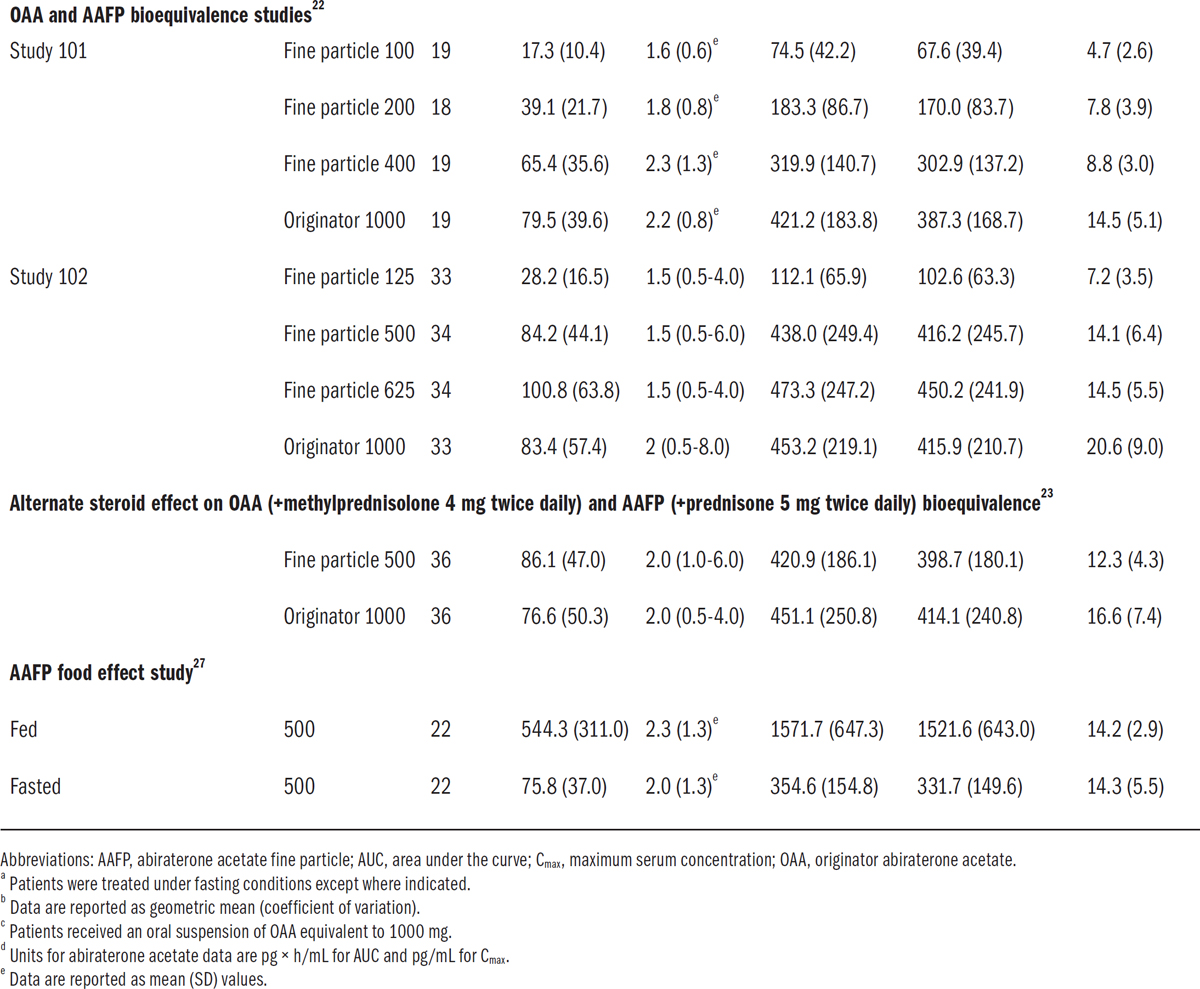
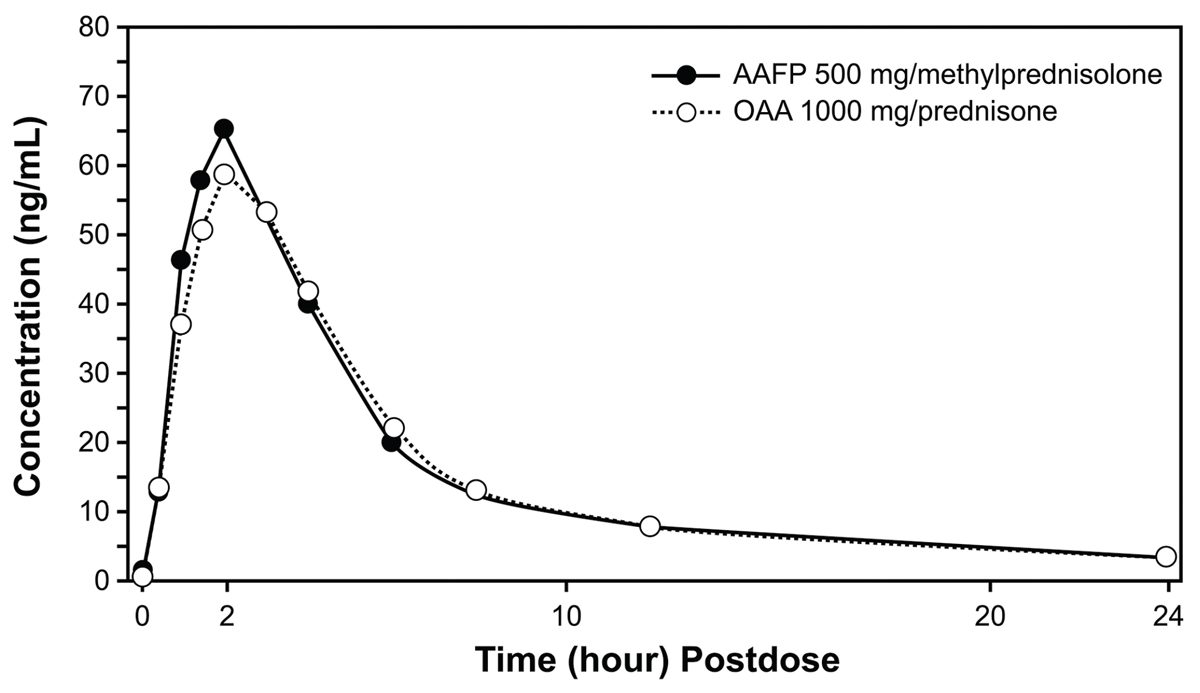
Various studies have reported pharmacokinetic parameters for OAA and AAFP formulation in healthy participants (Table 1) and patients with mCRPC (Table 2), with notably high interpatient and intrapatient variability. In healthy participants, the interpatient variability ranges from 32.7% to 119.8% for Cmax and 40.5% to 140.6% for the area under the concentration-time curve from 0 to infinity.9,20,21 In patients with metastatic and nonmetastatic CRPC, there is an interpatient variability of approximately 79% for Cmax and 64% for area under the curve (AUC) from 0 to 24 hours after multiple-day dosing vs 140% for Cmax and 107% for the AUC from 0 to 24 hours after a single dose.9,10,15 The bioequivalence of OAA 1000 mg and AAFP 500 mg was established in healthy participants under fasted conditions, indicating that a 50% lower dose of AAFP formulation produced equivalent pharmacokinetic parameters (area under the concentration-time curve from 0 to infinity, AUC from 0 to the time of the last quantifiable concentration, and Cmax ) to OAA22; results were later extended to show that specific steroid use (methylprednisolone vs prednisone) did not affect bioequivalence in healthy participants (Figure 2).23 Absorption of AAFP above the 500-mg dose was reported in the bioequivalence study, with a 625-mg dose having a higher Cmax and AUC than a 1000-mg dose of OAA.22 Originator abiraterone acetate absorption is conversely reported to be nearly saturated at the 1000-mg dose.20,22
Therapeutic equivalence of OAA 1000 mg and AAFP 500 mg administered once daily was also shown in patients with mCRPC in the randomized phase 2 STAAR study, based on a comparison of serum testosterone levels.12 The pharmacokinetic substudy from the STAAR study reported that pharmacokinetic parameters were not statistically different for AAFP and OAA in patients with mCRPC, though pharmacokinetic variability was high in both treatment groups.24 Safety findings were also similar across the 2 treatment groups in STAAR, further illustrating the potential clinical benefit of the lower dose of AAFP in patients with mCRPC.12
As demonstrated in multiple previous studies, food has a well-established effect on abiraterone absorption and disposition in healthy participants and patients with mCRPC.15,25 The presence of micelles and undigested lipids in the fed intestinal environment increases the solubility of abiraterone, resulting in a higher absorption of the drug in the fed than fasted state. A population pharmacokinetic model estimated that abiraterone bioavailability was 3.8 times higher when taken with a low-fat meal vs a fasted state and 7.6 times higher with a high-fat meal than in a fasted state, with high interpatient and intrapatient variability observed for various pharmacokinetic parameters.18 A relative bioavailability study in healthy participants showed that a formulation of abiraterone acetate in olive oil had a 4.5-fold higher exposure than standard tablets, underlining the effect a fatty environment can have on the bioavailability of abiraterone.9 Providing further evidence for this point, multiple phase 1 studies that examined patients with metastatic and nonmetastatic CRPC reported that OAA exposure increases 4.4-fold when administered with a high-fat meal compared with administration in a fasting state.15,25 In addition, healthy participants had statistically significant increases in abiraterone exposures, with Cmax values 7-fold and 17-fold higher following a low-fat or a high-fat meal, respectively, than when fasting. Area under the curve values showed similar statistically significant increases of 5-fold and 10-fold for a low-fat or high-fat meal, respectively, compared with fasting conditions.19 In the same report, however, the food effect was less pronounced for patients with mCRPC, with no appreciable effect on exposure observed for a low-fat meal compared with a fasting state, and there was only an approximately 2-fold increase in exposure for a high-fat meal vs fasting.19
Several factors may underlie the contrasting results between these studies, including differences in study design parameters, the small number of patients in the mCRPC cohort, the state of patients’ disease, the use of concomitant medications such as gonadotropin-releasing hormone analogs or low-dose prednisone in patients with mCRPC, and the difference in median age between the 2 groups (healthy participants, 37 years; patients with mCRPC, 70 years).19 The bioavailability of abiraterone may also be sensitive to the timing of food intake, with different exposure outcomes reported when healthy Japanese or White participants were given abiraterone 1 hour before a meal compared with 2 hours after a meal or when the participants received treatment between 2 meals consumed 4 hours apart.26 These results highlight that many factors can affect the bioavailability of abiraterone, including the population (healthy participants vs patients with mCRPC, who are also generally receiving concomitant medications that may potentially affect absorption or exposure), fed vs fasted state, and the timing of food intake.
Figure 2. Mean plasma abiraterone concentration-time plots are shown in patients on steady-state steroid and patients under fasted conditions for the pharmacokinetic population (linear scale)23Abbreviations: AAFP, abiraterone acetate fine particle; OAA, originator abiraterone acetate.Reproduced from Hussaini et al. Cancer Chemotherapy and Pharmacology. 80(3), 479-486. Reprinted with permission from Cancer Chemotherapy and Pharmacology (Copyright ©2017). Springer Nature. Reproduced without modification under Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Although less pronounced than for OAA, a food effect for AAFP formulation in healthy participants is also reported. In a randomized crossover study, the bioavailability of a 500-mg dose of AAFP increased in participants who consumed a high-fat meal 30 minutes before drug administration compared with its performance in fasting participants. Following a single dose of the AAFP formulation, the AUC and Cmax were 4.5-fold and 6.5-fold higher, respectively, under fed vs fasting conditions, and AAFP bioavailability was not bioequivalent for fed and fasting states.27 Abiraterone acetate fine particle formulation may nevertheless be taken with or without food per the US prescribing information whereas modified fasting conditions are specifically indicated for OAA (ie, no food intake 2 hours before and 1 hour after OAA administration).7,11
Clinical trials have examined various management strategies to address the food effect of abiraterone. One study compared a standard OAA regimen (1000 mg OAA, fasted) with a modified regimen (250 mg OAA with a low-fat meal) in patients with progressive CRPC.28 Although the primary efficacy end point was met (noninferiority of change from baseline serum prostate-specific antigen levels), these were statistically significant differences in pharmacokinetic parameters between the 2 regimens, with higher Cmax and trough levels for the standard regimen. A later crossover study in patients with mCRPC compared a standard 1000-mg fasted OAA regimen with a 500-mg OAA dose administered with a continental breakfast.10 Although Cmax and AUC values were similar for both treatment regimens, bioequivalence could not be established, and the trial was terminated. Real-world data from a therapeutic drug monitoring (TDM) program assessed whether pharmacokinetics-guided dosing with food was a feasible approach to achieve a threshold minimum abiraterone serum concentration in patients with mCRPC and metastatic hormone-sensitive prostate cancer.29 Compared with a before-food intervention (light meal or snack, not standardized), higher exposure levels were observed in patients with low pretreatment trough levels (minimum serum concentration of 8.4 ng/mL) who received abiraterone administration with concomitant food intake.29 Monitoring abiraterone levels in combination with a food intervention may therefore represent a costeffective approach to treatment.
Alternate formulations of abiraterone acetate have been developed in an attempt to alleviate the known food effect of OAA.30-35 Although promising early results were reported with an abiraterone formulation produced using continuous flow precipitation,34,35 a later formulation from the same research group developed as an oral suspension did not achieve comparable serum concentrations 24 hours after the dose when administered in a modified prandial state to individuals observed with OAA administered in the fasted state.32 Thus far, additional iterations of abiraterone, including an amorphous solid dispersion,31 a multicomponent crystal form,33 and a tablet coformulated with the absorption enhancer sodium N-(8-[2-hydroxybenzoyl] amino) caprylate30 are reported only in preclinical or phase 1 studies. Further studies are therefore needed to determine the long-term effects of this approach.
The medication burden for patients treated with oral anticancer medications can be substantial; lower doses have the potential to reduce the occurrence of AEs and toxicity. In patients with mCRPC, abiraterone is associated with an increased risk of cardiovascular disease (CVD), including ischemic heart disease, myocardial infarction, supraventricular tachyarrhythmias, ventricular tachyarrhythmias, cardiac failure, and arrhythmia.36 In the STAMPEDE trial (ClinicalTrials.gov identifier NCT00268476) in patients with metastatic prostate cancer, cardiovascular AEs were the second-most reported AE of grade 3 or higher following endocrine disorders; cardiovascular AEs occurred in 10% of those patients in the abiraterone plus ADT arm vs 4% of those in the ADT monotherapy arm.37 In a population-based Swedish study, compared with control patients who received only gonadotropinreleasing hormone agonists, increased risk of CVD was reported for patients with mCRPC treated with abiraterone plus gonadotropin-releasing hormone agonists.36 Consistent with these findings, several meta-analyses of patients with prostate cancer have reported increased all-grade and high-grade CVD risk with abiraterone compared with control individuals not treated with abiraterone,38,39 with a higher risk of mortality in patients with preexisting CVD who received abiraterone than in patients without preexisting CVD.40 Patients in the STAMPEDE trial who received OAA also experienced more grade 3 to 5 musculoskeletal events than patients who received ADT alone37; conversely, in the STAAR study, any-grade musculoskeletal events occurred less frequently in patients in the AAFP group (12.5%) vs the OAA group (37.9%).12 In addition to these specific events, AEs of any type but grade 3 or higher generally occurred more frequently in phase 2 and 3 trials with OAA than with the reference treatment.5,6,37 Further controlled clinical studies are needed to explore whether receiving lower doses of abiraterone acetate may mitigate the risk of AEs, including CVD, in patients with prostate cancer. It is crucial, however, to ensure that patients receive a sufficient dose to achieve therapeutic efficacy. Ideally, strategies such as TDM can be used for that purpose, but they require substantial resources and can increase treatment costs.41 The use of AAFP may improve the therapeutic window of abiraterone acetate compared with OAA and can therefore represent a more pragmatic and cost-effective alternative to TDM to achieve therapeutic efficacy with reduced drug doses.
Despite being an efficacious and well-tolerated treatment for mCRPC, OAA is a biopharmaceutical classification system class IV drug with poor solubility and bioavailability and an established food effect. Abiraterone acetate fine particle formulation was designed to partially alleviate the solubility, pharmacokinetic variability, and food effect issues associated with OAA while maintaining bioequivalence in terms of efficacy and safety. Although a food effect is also observed with AAFP formulation, its magnitude is less than that reported for OAA. Increased exposure to abiraterone is linked to slower disease progression, longer overall survival, and mitigation of CYP17 inhibition resistance, providing an efficacy rationale and potential impetus to increase drug exposure. Using AAFP formulation can facilitate the attainment of an abiraterone acetate dose within the therapeutic window and improve the predictability of abiraterone acetate absorption. This approach may improve safety and overall outcomes and avoid the need for costly strategies such as TDM in patients with mCRPC, lowering patients’ total treatment costs more effectively than OAA. Future studies should add to the available data that suggest an improved risk-benefit ratio for AAFP compared with OAA.
Age-standardized rate (world) per 100 000, incidence, males, in 2022. International Agency for Research on Cancer. Updated February 8, 2024. Accessed July 2, 2025. https://gco.iarc.who.int/today/en/dataviz/bars?mode=cancer&group_populations=1&sexes=1&include_nmsc=1&include_nmsc_other=0&types=0&group_crc=0
Desai MM, Cacciamani GE, Gill K, et al. Trends in incidence of metastatic prostate cancer in the US. JAMA Netw Open. 2022;5(3):e222246. doi:10.1001/jamanetworkopen.2022.2246
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines® ): Prostate Cancer. Version 2.2025. Updated April 16, 2025. Accessed July 2, 2025. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
Parker C, Castro E, Fizazi K, et al; ESMO Guidelines Committee. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(9):1119-1134. doi:10.1016/j.annonc.2020.06.011
Fizazi K, Tran NP, Fein L, et al; LATITUDE Investigators. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-360. doi:10.1056/NEJMoa1704174
Ryan CJ, Smith MR, de Bono JS, et al; COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138-148. doi:10.1056/NEJMoa1209096
Zytiga. Prescribing information. Janssen Biotech, Inc; 2024. Accessed August 13, 2025. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/ZYTIGA-pi.pdf
Auchus RJ, Yu MK, Nguyen S, Mundle SD. Use of prednisone with abiraterone acetate in metastatic castration-resistant prostate cancer. Oncologist. 2014;19(12):1231-1240. doi:10.1634/theoncologist.2014-0167
NDA 202-379 review—abiraterone acetate. US Food and Drug Administration Center for Drug Evaluation and Research. Application No. 202379Orig1s000. December 20, 2010. Accessed May 3, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/202379orig1s000clinpharmr.pdf
Lubberman FJE, Benoist GE, Gerritsen W, et al. A prospective phase I multicentre randomized cross-over pharmacokinetic study to determine the effect of food on abiraterone pharmacokinetics. Cancer Chemother Pharmacol. 2019;84(6):1179-1185. doi:10.1007/s00280-019-03952-w
Yonsa. Prescribing information. Sun Pharmaceutical Industries, Inc; 2022. Accessed August 13, 2025. https://www.yonsarx.com/PI.pdf
Stein CA, Levin R, Given R, et al. Randomized phase 2 therapeutic equivalence study of abiraterone acetate fine particle formulation vs. originator abiraterone acetate in patients with metastatic castration-resistant prostate cancer: the STAAR study. Urol Oncol. 2018;36(2):81.e9-81.e16. doi:10.1016/j.urolonc.2017.10.018
Chapas-Reed J, Stein C, Squittieri N, Concepcion R. Oneyear, open-label extension study on the safety and efficacy of abiraterone acetate fine particle formulation in patients with metastatic castration-resistant prostate cancer. Clin Med Insights Urol. 2020;13. doi:10.1177/1179561120910125
Danielak D, Krejčí T, Beránek J. Increasing the efficacy of abiraterone—from pharmacokinetics, through therapeutic drug monitoring to overcoming food effects with innovative pharmaceutical products. Eur J Pharm Sci. 2022;176:106254. doi:10.1016/j.ejps.2022.106254
Ryan CJ, Smith MR, Fong L, et al. Phase I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating clinical activity in patients with castration-resistant prostate cancer who received prior ketoconazole therapy. J Clin Oncol. 2010;28(9):1481-1488. doi:10.1200/JCO.2009.24.1281
Acharya M, Gonzalez M, Mannens G, et al. A phase I, open-label, single-dose, mass balance study of 14C-labeled abiraterone acetate in healthy male subjects. Xenobiotica. 2013;43(4):379-389. doi:10.3109/00498254.2012.721022
Marbury T, Lawitz E, Stonerock R, et al. Single-dose pharmacokinetic studies of abiraterone acetate in men with hepatic or renal impairment. J Clin Pharmacol. 2014;54(7):732-741. doi:10.1002/jcph.253
Stuyckens K, Saad F, Xu XS, et al. Population pharmacokinetic analysis of abiraterone in chemotherapy-naive and docetaxel-treated patients with metastatic castration-resistant prostate cancer. Clin Pharmacokinet. 2014;53(12):1149-1160. doi:10.1007/s40262-014-0178-6
Chi KN, Spratlin J, Kollmannsberger C, et al. Food effects on abiraterone pharmacokinetics in healthy subjects and patients with metastatic castration-resistant prostate cancer. J Clin Pharmacol. 2015;55(12):1406-1414. doi:10.1002/jcph.564
Assessment report for Zytiga (abiraterone). European Medicines Agency. Report No. EMA/CHMP/542871/2011. July 21, 2011. Accessed May 3, 2024. https://www.ema.europa.eu/en/documents/assessment-report/zytiga-epar-public-assessment-report_en.pdf
Benoist GE, Hendriks RJ, Mulders PFA, et al. Pharmacokinetic aspects of the two novel oral drugs used for metastatic castration-resistant prostate cancer: abiraterone acetate and enzalutamide. Clin Pharmacokinet. 2016;55(11):1369-1380. doi:10.1007/s40262-016-0403-6
Goldwater R, Hussaini A, Bosch B, Nemeth P. Comparison of a novel formulation of abiraterone acetate vs. the originator formulation in healthy male subjects: two randomized, open-label, crossover studies. Clin Pharmacokinet. 2017;56(7):803-813. doi:10.1007/s40262-017-0536-2
Hussaini A, Olszanski AJ, Stein CA, Bosch B, Nemeth P. Impact of an alternative steroid on the relative bioavailability and bioequivalence of a novel versus the originator formulation of abiraterone acetate. Cancer Chemother Pharmacol. 2017;80(3):479-486. doi:10.1007/s00280-017-3360-3
Dunshee C, Stein CA, Nemeth PR, Bosch B, Chapas-Reed J, Dreicer R. Pharmacokinetic (PK) subgroup results from the phase 2 pharmacodynamic and bioequivalence study of abiraterone acetate fine particle formulation (AAFP) in patients with metastatic castration-resistant prostate cancer (mCRPC): the STAAR study. J Clin Oncol. 2018;36(6_suppl):176. doi:10.1200/JCO.2018.36.6_suppl.176
Attard G, Reid AHM, Yap TA, et al. Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol. 2008;26(28):4563-4571. doi:10.1200/JCO.2007.15.9749
Inoue K, Shishido A, Vaccaro N, et al. Pharmacokinetics of abiraterone in healthy Japanese men: dose-proportionality and effect of food timing. Cancer Chemother Pharmacol. 2015;75(1):49-58. doi:10.1007/s00280-014-2616-4
Papangelou A, Olszanski AJ, Stein CA, Bosch B, Nemeth P. The effect of food on the absorption of abiraterone acetate from a fine particle dosage form: a randomized crossover trial in healthy volunteers. Oncol Ther. 2017;5:161-170. doi:10.1007/s40487-017-0054-2
Szmulewitz RZ, Peer CJ, Ibraheem A, et al. Prospective international randomized phase II study of low-dose abiraterone with food versus standard dose abiraterone in castration-resistant prostate cancer. J Clin Oncol. 2018;36(14):1389-1395. doi:10.1200/JCO.2017.76.4381
Groenland SL, van Nuland M, Bergman AM, et al; Dutch Pharmacology Oncology Group (DPOG). Concomitant intake of abiraterone acetate and food to increase pharmacokinetic exposure: real life data from a therapeutic drug monitoring programme. Eur J Cancer. 2020;130:32-38. doi:10.1016/j.ejca.2020.02.012
Feng Z, Liu Y, Kuang Y, et al. Open-label, phase I, pharmacokinetic studies in healthy Chinese subjects to evaluate the bioequivalence and food effect of a novel formulation of abiraterone acetate tablets. Drug Des Devel Ther. 2022;16:3-12. doi:10.2147/DDDT.S339305
Gala U, Miller D, Williams RO III. Improved dissolution and pharmacokinetics of abiraterone through KinetiSol® enabled amorphous solid dispersions. Pharmaceutics. 2020;12(4):357. doi:10.3390/pharmaceutics12040357
Jordán T, Basa-Dénes O, Angi R, et al. Dose finding and food effect studies of a novel abiraterone acetate formulation for oral suspension in comparison to a reference formulation in healthy male subjects. Pharmaceutics. 2021;13(12):2171. doi:10.3390/pharmaceutics13122171
Silveira RG, Cunha BN, Tenório JC, et al. A simple alternative to prodrug: the hydrochloride salt monohydrate of the prostate anticancer drug abiraterone. J Mol Struct. 2019;1190:165-170. doi:10.1016/j.molstruc.2019.04.068
Solymosi T, Ötvös Z, Angi R, et al. Novel formulation of abiraterone acetate might allow significant dose reduction and eliminates substantial positive food effect. Cancer Chemother Pharmacol. 2017;80(4):723-728. doi:10.1007/s00280-017-3406-6
Solymosi T, Ötvös Z, Angi R, et al. Development of an abiraterone acetate formulation with improved oral bioavailability guided by absorption modeling based on in vitro dissolution and permeability measurements. Int J Pharm. 2017;532(1):427-434. doi:10.1016/j.ijpharm.2017.09.031
George G, Vikman H, Gedeborg R, et al. Risk of cardiovascular events in men on abiraterone or enzalutamide combined with GnRH agonists: nation-wide, population-based cohort study in Sweden. Acta Oncol. 2021;60(4):459-465. doi:10.1080/0284186X.2021.1885058
James ND, de Bono JS, Spears MR, et al; STAMPEDE Investigators. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. 2017;377(4):338-351. doi:10.1056/NEJMoa1702900
Moreira RB, Debiasi M, Francini E, et al. Differential side effects profile in patients with mCRPC treated with abiraterone or enzalutamide: a meta-analysis of randomized controlled trials. Oncotarget. 2017;8(48):84572-84578. doi:10.18632/oncotarget.20028
Iacovelli R, Ciccarese C, Bria E, et al. The cardiovascular toxicity of abiraterone and enzalutamide in prostate cancer. Clin Genitourin Cancer. 2018;16(3):e645-e653. doi:10.1016/j.clgc.2017.12.007
Lu-Yao G, Nikita N, Keith SW, et al. Mortality and hospitalization risk following oral androgen signaling inhibitors among men with advanced prostate cancer by pre-existing cardiovascular comorbidities. Eur Urol. 2020;77(2):158-166. doi:10.1016/j.eururo.2019.07.031
Liang WS, Beaulieu-Jones B, Smalley S, Snyder M, Goetz LH, Schork NJ. Emerging therapeutic drug monitoring technologies: considerations and opportunities in precision medicine. Front Pharmacol. 2024;15:1348112. doi:10.3389/fphar.2024.1348112
Bouhajib M, Tayab Z. Evaluation of the pharmacokinetics of abiraterone acetate and abiraterone following single-dose administration of abiraterone acetate to healthy subjects. Clin Drug Investig. 2019;39(3):309-317. doi:10.1007/s40261-019-00752-1
Massard C, Mateo J, Loriot Y, et al. Phase I/II trial of cabazitaxel plus abiraterone in patients with metastatic castration-resistant prostate cancer (mCRPC) progressing after docetaxel and abiraterone. Ann Oncol. 2017;28(1):90-95. doi:10.1093/annonc/mdw441
Tagawa ST, Posadas EM, Bruce J, et al. Phase 1b study of abiraterone acetate plus prednisone and docetaxel in patients with metastatic castration-resistant prostate cancer. Eur Urol. 2016;70(5):718-721. doi:10.1016/j.eururo.2016.01.028
Published: October 5, 2025.
Conflict of Interest Disclosures: A. Guminski has participated on advisory boards for Bristol Myers Squibb, Pfizer, and Sanofi; received honoraria from Novartis; and received travel support from Astellas Pharma and Bristol Myers Squibb. C. M. Pieczonka reports ownership of stock and other ownership interests from US Urology Partners; honoraria from AstraZeneca, Bayer, Bristol Myers Squibb, Dendreon, Janssen, Merck, Myovant Sciences, Novartis, Pfizer/Astellas, and Sun Pharma; participation as an advisor or consultant for AstraZeneca, Bayer, Bristol Myers Squibb, Dendreon, Janssen Oncology, Merck, Novartis, Pfizer/Astellas, Sun Pharma, and Tolmar; membership in the speakers’ bureau of Astellas Pharma, AstraZeneca, Bayer, Dendreon, Janssen Oncology, Merck, Myovant Sciences, Pfizer, and Sun Pharma; and research funding from Advantagene, Astellas Pharma, AstraZeneca, Bayer, Dendreon, InVitae, Janssen Oncology, Merck, and Pfizer. B. A. Mehlhaff reports honoraria, travel accommodations, and participation as an advisor or consultant for Amgen, Astellas Pharma, Bayer, Janssen, and Pfizer and grants and funding from Astellas Pharma, Bayer, Janssen, and Pfizer. A. Fojo was the editor for Seminars in Oncology during development of this manuscript. A. M. Joshua reports participation as an advisor or consultant (to their institution) for Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Eisai, Ipsen, Janssen Oncology, Merck Serono, Novartis, Pfizer, and Sanofi and research funding (to their institution) from AstraZeneca, Bayer, Bristol Myers Squibb, Genentech, Janssen Oncology, Lilly, Mayne Pharma, Merck Sharp & Dohme, and Pfizer.
Funding/Support: Medical writing and editorial support were provided by Juliette M. Bouyssou, PhD, of Red Nucleus and funded by Sun Pharmaceutical Industries, Inc.
Author Contributions: All authors meet the criteria for authorship set forth by the International Committee for Medical Journal Editors and have significantly contributed to, reviewed, and approved the final submitted version of this manuscript.
Data Availability Statement: All data sources are cited and publicly available or available upon reasonable request to the corresponding author.
Acknowledgments: Medical writing and editorial support were provided by Juliette M. Bouyssou, PhD, of Red Nucleus.
Citation: Guminski A, Pieczonka CM, Mehlhaff BA, Fojo A, Joshua AM. Food effect of abiraterone acetate in patients with prostate cancer. Rev Urol. 2025;24(3):e39-e50.
Corresponding author: Alexander Guminski, Northern Clinical School, Faculty of Medicine and Health, University of Sydney, Science Rd, Camperdown NSW 2050, Australia (alexander.guminski@sydney.edu.au)