Cancer Chemotherapy Update
Lenvatinib and Palbociclib
Dominic A. Solimando, Jr, MA, FAPhA, FASHP, BCOP, and J. Aubrey Waddell, PharmD, FAPhA, BCOP
Cancer Chemotherapy Update
Lenvatinib and Palbociclib
Dominic A. Solimando, Jr, MA, FAPhA, FASHP, BCOP, and J. Aubrey Waddell, PharmD, FAPhA, BCOP
Cancer Chemotherapy Update
Lenvatinib and Palbociclib
Dominic A. Solimando, Jr, MA, FAPhA, FASHP, BCOP, and J. Aubrey Waddell, PharmD, FAPhA, BCOP
The complexity of cancer chemotherapy requires pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparation, dispensing, and administration of antineoplastic therapy, and the agents, both commercially available and investigational, used to treat malignant diseases. Questions or suggestions for topics should be addressed to Dominic A. Solimando, Jr, President, Oncology Pharmacy Services, Inc., 4201 Wilson Blvd #110-545, Arlington, VA 22203, e-mail: OncRxSvc@comcast.net; or J. Aubrey Waddell, Professor, University of Tennessee College of Pharmacy; Oncology Pharmacist, Pharmacy Department, Blount Memorial Hospital, 907 E. Lamar Alexander Parkway, Maryville, TN 37804, e-mail: waddfour@charter.net.
Name: Lenvatinib
Synonyms: Lenvima; E7080
The complexity of cancer chemotherapy requires pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparation, dispensing, and administration of antineoplastic therapy, and the agents, both commercially available and investigational, used to treat malignant diseases. Questions or suggestions for topics should be addressed to Dominic A. Solimando, Jr, President, Oncology Pharmacy Services, Inc., 4201 Wilson Blvd #110-545, Arlington, VA 22203, e-mail: OncRxSvc@comcast.net; or J. Aubrey Waddell, Professor, University of Tennessee College of Pharmacy; Oncology Pharmacist, Pharmacy Department, Blount Memorial Hospital, 907 E. Lamar Alexander Parkway, Maryville, TN 37804, e-mail: waddfour@charter.net.
Name: Lenvatinib
Synonyms: Lenvima; E7080
The complexity of cancer chemotherapy requires pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparation, dispensing, and administration of antineoplastic therapy, and the agents, both commercially available and investigational, used to treat malignant diseases. Questions or suggestions for topics should be addressed to Dominic A. Solimando, Jr, President, Oncology Pharmacy Services, Inc., 4201 Wilson Blvd #110-545, Arlington, VA 22203, e-mail: OncRxSvc@comcast.net; or J. Aubrey Waddell, Professor, University of Tennessee College of Pharmacy; Oncology Pharmacist, Pharmacy Department, Blount Memorial Hospital, 907 E. Lamar Alexander Parkway, Maryville, TN 37804, e-mail: waddfour@charter.net.
Name: Lenvatinib
Synonyms: Lenvima; E7080
Hosp Pharm 2015;50(7):578–582
2015 © Thomas Land Publishers, Inc.
doi: 10.1310/hpj5007-578
MECHANISM OF ACTION
Lenvatinib is a tyrosine kinase inhibitor that reacts with a number of targets including vascular endothelial growth factor receptor (VEGFR)-1 (Flt-1), VEGFR-2 (KDR), VEGFR-3 (Flt-4), fibroblast growth factor receptor (FGFR)-1, platelet-derived growth factor (PDGF) β, and c-KIT. Lenvatinib decreases phosphorylation of VEGFR-2 and inhibits the growth of vascular endothelial cells and formation of vascular-like structures.1-3
PHARMACOKINETICS
Over a dose range of 0.5 mg to 20 mg orally (PO) twice a day, the time to maximum concentration (Tmax) ranges from 1 to 5 hours; the maximum concentration (Cmax) is 2.5 ng/mL to 674 ng/mL.4 The 24-hour area under the time versus concentration curve (AUC) was 41 ng•h/mL to 4751 ng•h/mL.4 The elimination half-life (T½) was 46.9 hours to 31.6 hours.4
For single daily oral doses of 0.2 mg to 32 mg, the Tmax was 1.5 to 6.4 hours; the Cmax was 0.7 to 681.5 ng/mL.5 The 24-hour AUC was 14.0 ng•h/mL to 5093.5 ng•h/mL.5 The T½ was 5.3 to 18.2 hours.5
For oral doses of 4 or 6 mg twice daily, the mean Tmax was 4.18 and 4.27 hours; the Cmax was 97.5 and 138 ng/mL respectively.6 The mean AUC was 692 ng•h/mL and 848 ng•h/mL.6
The capsule formulation is reported to have about 10% lower Cmax and 14% lower AUC than the tablet formulation.7
Following continuous oral dosing with 24 mg daily, the Tmax is 1 to 4 hours; following a high-fat meal, this is delayed to 2 to 4 hours. The AUC increased proportionally with dose from 3.2 to 32 mg. Lenvatinib is 98% to 99% protein bound. Lenvatinib is metabolized in the liver, primarily by CYP3A and aldehyde oxidase. Sixty-four percent is excreted in the feces; 25% is excreted in the kidney. The elimination half-life (T½) is 28 hours.8 Lenvatinib is highly (97% to 99%) protein-bound.4,8
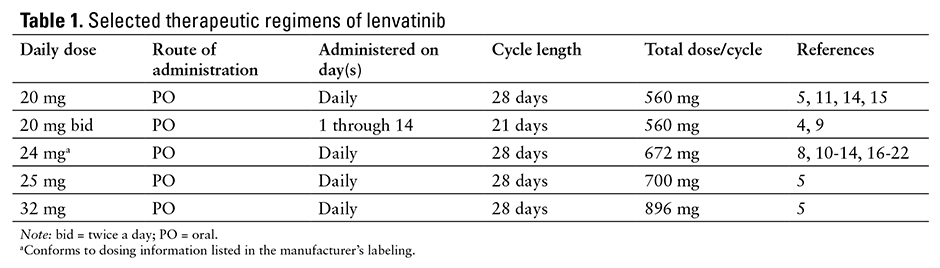
Selected therapeutic regimens of lenvatinib appear in Table 1.
PREPARATION
- Lenvatinib is available as 4 mg and 10 mg capsules.
- The product is packaged in 5-day dose cards of 10 mg, 14 mg, 20 mg, and 24 mg/day.
STABILITY
- The drug should be stored at room temperature 25°C (77°F).
- Brief (less than 24 hours) exposure to temperatures up to 30°C (86°F) is acceptable.
ADMINISTRATION
- Lenvatinib is administered orally; usually once a day.
- Administration with a high-fat meal has no effect on overall AUC, but absorption is slowed.7
- Lenvatinib can be administered with, or without, food.7,8
TOXICITIES (24 mg daily)
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf). Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities but make, or consider making, dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
- Cardiovascular: Edema, peripheral 11%,18 (grade 3 or 4) 0.4%18; hypertension 48% to 68%,13,15-17 (grade 3) 4% to 17%,13,15,19 (grade 3 or 4) 33% to 42%.15,17,18
- Central Nervous System: Headache 26% to 27%,17,18 (grade 3 or 4) 1% to 3%.17,18
- Constitutional: Dysphonia 24% to 27%,17,18 (grade 3 or 4) 1%18; fatigue 42% to 100%,10,11,13,15-18 (grade 3) 5% to 13%,11,13,15,16 (grade 3 or 4) 9% to 42%17,18; weight loss 32% to 46%,13,15,18 (grade 3) 3% to 4%,13,15 (grade 3 or 4) 10%.18
- Dermatologic: Alopecia 11%18; rash 16% to 50%,10,18 (grade 3 or 4) 0.4%.18
- Endocrine/Metabolic: Hypocalcemia 7%,18 (grade 3 or 4) 3%18; hypothyroidism 46%.11
- Gastrointestinal: Anorexia 35% to 50%,10,11,13,16-18 (grade 3) 2% to 5%,13,15,16 (grade 3 or 4) 5%18; constipation 15% to 50%,10,18 (grade 3 or 4) 0.4%18; diarrhea 35% to 59%,10,11,13,15-18 (grade 3) 5%,11,13,15,16 (grade 3 or 4) 2% to 8%17,18; dysgeusia 17%18; dyspepsia 10%18; mucosal inflammation 100%10; nausea 32% to 50%,10,11,16-18 (grade 3) 3%,16 (grade 3 or 4) 2% to 3%17,18; stomatitis 36%,18 (grade 3 or 4) 4%18; vomiting 28% to 50%,10,11,18 (grade 3) 2%,17 (grade 3 or 4) 2%18; xerostomia 14%,18 (grade 3 or 4) 0.4%.18
- Hematologic: Thrombocytopenia 32%.11
- Infection: Pneumonia (grade 3 or 4) 9%.19
- Musculoskeletal: Arthralgia 18%18; myalgia 15%,18 (grade 3 or 4) 2%.18
- Neurologic: Palmar-plantar erythrodysesthesia 32%,18 (grade 3 or 4) 3%.18K. Pain: Abdominal 12%,18 (grade 3 or 4) 0.4%18; oropharyngeal 10%,18 (grade 3 or 4) 0.4%18; upper abdominal 13%.18
- Pulmonary: Dyspnea 50%,10 (grade 3 or 4) 9%19; embolism (grade 3 or 4) 3%.18
- Renal: Proteinuria 26% to 58%,11,13,15,17,18 (grade 3) 2% to 7%,13,15 (grade 3 or 4) 4% to 10%.17,18
DOSE ADJUSTMENT
A. Hepatic
- Mild or moderate hepatic impairment, no dose adjustment is required.8
- Severe hepatic impairment, reduce dose to 14 mg daily.8
- Child-Pugh A or B, reduce dose to 10 mg daily.20,21
- Child-Pugh C, reduce dose to 8 mg daily.20
- Due to the limited number of dosage forms commercially available, the recommended 8 mg and 12 mg doses would be difficult to administer.
B. Renal
- Mild or moderate renal impairment, no dose adjustment is required.8
- Severe renal impairment, reduce dose to 14 mg daily.8
Name: Palbociclib
Synonyms: Ibrance; PD 0332991
MECHANISM OF ACTION
Cyclin dependent kinases (CDK) 4 and 6, with cyclin D (an activating subunit), promote progression of the cell cycle from the G1 to the S phase by phosphorylating the retinoblastoma (Rb) protein.22 Palbociclib is a reversible inhibitor of CDK 4 and 6. Inhibition of CDK 4 and 6 by palbociclib results in cell-cycle arrest in the G1 phase.23,24
PHARMACOKINETICS
For doses of 100 mg to 225 mg daily, the mean Tmax was 4 to 7 hours; the Cmax was 44 to 186 ng/mL.25 The AUC was 333 to 1491 ng•h/mL.25
For single doses of 25 mg to 150 mg, the Tmax was 4 to 7 hours; Cmax was 10 to 91 ng/mL.26 The AUC was 58 to 641 ng•h/mL.26 For daily doses of 25 mg to 150 mg/day, the Tmax was 4 to 7 hours; Cmax was 16 to 128 ng/mL.26 The AUC was 119 to 1084 ng•h/mL.26
The volume of distribution (Vd) is2583 L; the drug is 85% protein bound. Palbociclib is metabolized in the liver primarily by oxidation and sulfonation via CYP3A and SULT2A1; acylation and glucuronidation also occur. The major metabolite in circulation is glucuronide palbociclib conjugate. About 17.5% of a dose is excreted renally, primarily as metabolites. About 74.1% is excreted in the feces, primarily as sulfamic acid palbociclib conjugate. Oral clearance of palbociclib is 63.1 L/h; the mean plasma T½ is 29 hours.27
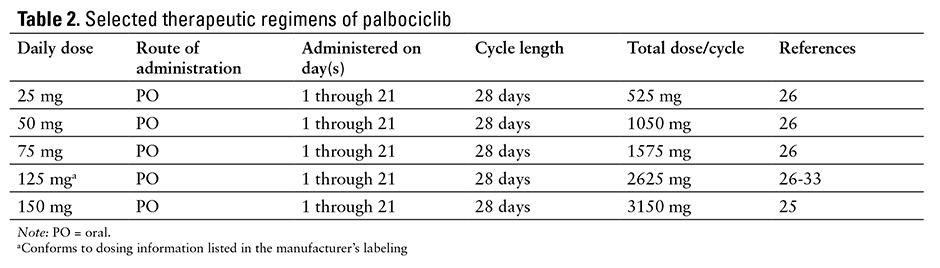
Selected therapeutic regimens of palbociclib appear in Table 2.
PREPARATION
- Palbociclib is available as 75 mg, 100 mg, and 125 mg capsules.
STABILITY
- The drug should be stored at room temperature 20ºC to 25°C (68º to 77°F).
- Brief (less than 24 hours) exposure to temperatures between 15º and 30°C (59º to 86°F) is acceptable.
ADMINISTRATION
- Palbociclib is administered orally; usually once a day.
- Palbociclib should be taken with food.
- Patients should be advised to avoid grapefruit and grapefruit juice.
TOXICITIES (125 mg days 1 through 21 every 28 days)
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf). Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities but make, or consider making, dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
- Central Nervous System: Dizziness 10% to 12%28,29; headache 12% to 14%.28,29
- Constitutional: Asthenia 11%,29 (grade 3) 2%29; fatigue 35% to 36%,28,29 (grade 3) 2%,29 (grade 4) 2%29; hot flush 21%.29
- Dermatologic: Alopecia 22%.29
- Endocrine/Metabolic: Hypophosphatemia (grade 3) 12%.28
- Hematologic: Anemia 12% to 29%,28,29 (grade 3) 5%,29 (grade 4) 1%29; epistaxis 11%29; leukopenia 12% to 24%,28,29 (grade 3) 19%,29 (grade 4) 6%28; neutropenia 20% to 41%,28,29 (grade 3) 24% to 40%,28,29,31 (grade 3 or 4) 19%,30 (grade 4) 6% to 12%28,29; neutropenic fever (grade 3) 6%33; thrombocytopenia 14% to 29%,28,29 (grade 3) 2% to 18%,28-30 (grade 4) 6%.28
- Gastrointestinal: Anorexia 14%,29 (grade 3) 1%29; constipation 12%29; diarrhea 17% to 18%,28,29 (grade 3) 4% to 6%28,29; nausea 12% to 23%,28,29 (grade 3) 2%29; stomatitis 12%29; vomiting 14%.29
- Hepatic: Increased alanine aminotransferase (ALT) and aspartate aminotransferase (AST) (grade 3) 11%33; transaminitis (grade 3 or 4) 6%.30
- Infection: Influenza 10%,29 (grade 3) 1%29; upper respiratory tract 10%,29 (grade 3) 1%.29
- Musculoskeletal: Arthralgia 22%,29 (grade 3) 1%29; rhabdomyolitis (grade 3 or 4) 6%.29
- Neurologic: Peripheral neuropathy 10%.29
- Oral: Nasopharygitis16%.29
- Pain: Back 13%,29 (grade 4) 1%29; bone 10%,29 (grade 3) 1%,29 (grade 4) 1%29; in extremity 10%29; musculoskeletal 10%,29 (grade 3) 1%29; oropharyngeal 10%.29
- Pulmonary: Cough 12%29; dyspnea 13%,29 (grade 3) 2%.29
DOSE ADJUSTMENT
A. Hepatic
- Bilirubin less than or equal to the upper limit of normal (ULN) and AST greater than the ULN, no dose adjustment required.27
- Bilirubin greater than 1 to 1.5 times the ULN, no dose adjustment required.27
- Bilirubin greater than 1.5 times the ULN, no information available.27
B. Renal
- Creatinine clearance greater than or equal to 60 mL/min, no dose adjustment required.27
- Creatinine clearance less than 60 mL/min, no information available.27
REFERENCES
- Matsui J, Yamamoto Y, Funahashi Y, et al. E7080, a novel inhibitor that targets multiple kinases, has potent antitumor activities against stem cell factor producing human small cell lung cancer H146, based on angiogenesis inhibition. Int J Cancer. 2008;122(3):664-671.
- Matsui J, Funahashi Y, Uenaka T et al. Multi-kinase inhibitor E7080 suppresses lymph node and lung metastases of human mammary breast tumor MDA-MB-231 via inhibition of vascular endothelial growth factor (VEGF-R) 2 and VEGF-R3 kinase. Clin Cancer Res. 2008;14(17):5458-5465.
- Ikulta K, Yano S, Trung VT, et al. E7080, a multi-tyrosine kinase inhibitor, suppresses the progression of malignant pleural mesothelioma with different proangiogenic cytokine production profiles. Clin Cancer Res. 2009;15(23):7229-7239.
- Yamada K, Yamamoto N, Yamada Y, et al. Phase I dose-escalation study and biomarker analysis of E7080 in patients with advanced solid tumors. Clin Cancer Res. 2011;17(8):2528-2537.
- Boss DS, Glen H, Beijnen JH, et al. A phase I study of E7080, a multitargeted tyrosine kinase inhibitor, in patients with advanced solid tumours. Br J Cancer. 2012;106(10):1598-1604.
- Nishio M, Horai T, Horiike A, et al. Phase 1 study of lenvatinib combined with carboplatin and paclitaxel in patients with non-small-cell lung cancer. Br J Cancer. 2013;109(3):538-544.
- Shumaker R, Aluri J, Fan J, et al. Evaluation of the effects of formulation and food on the pharmacokinetics of lenvatinib (E7080) in healthy volunteers. Int J Clin Pharmacol Ther. 2014;52(4):284-291.
- Lenvima [prescribing information]. Woodcliff Lake, NJ: Eisai Inc; 2015.
- Koyama N, Saito K, Nishioka Y, et al. Pharmacodynamic change in plasma angiogenic proteins: A dose-escalation phase 1 study of the multi-kinase inhibitor lenvatinib. BMC Cancer. 2014;14:530.
- Molina AM, Hutson TE, Larkin J, et al. A phase 1b clinical trial of the multi-targeted tyrosine kinase inhibitor lenvatinib (E7080) in combination with everolimus for treatment of metastatic renal cell carcinoma (RCC). Cancer Chemother Pharmacol. 2014;73(1):181-189.
- Hong DA, Andresen C, Mink J, et al. A phase IB study of lenvatinib (E7080) in combination with temozolomide for treatment of advanced melanoma. Proc Am Soc Clin Oncol. 2012. Abstract 8594. http://meetinglibrary.asco.org/content/101118-114. Accessed March 10, 2015.
- Maio M, Hassel JC, Del Vecchio M, et al. Lenvatinib combined with dacarbazine versus dacarbazine alone as first-line treatment in patients with stage IV melanoma. Proc Am Soc Clin Oncol. 2013. Abstract 9027. http://meetinglibrary.asco.org/content/115263-132. Accessed March 10, 2015.
- Sherman SI, Jarzab B, Cabanillas ME, et al. A phase II trial of the multitargeted kinase inhibitor E7080 in advanced radioiodine (RAI)-refractory differentiated thyroid cancer (DTC). Proc Am Soc Clin Oncol. 2011. Abstract 5503. http://meetinglibrary.asco.org/content/73708-102. Accessed March 10, 2015.
- Ball DW, Sherman SI, Jarzab B, et al. Lenvatinib treatment of advanced RAI-refractory differentiated thyroid cancer (DTC): Cytokine and angiogenic factor (CAF) profiling in combination with tumor genetic analysis to identify markers associated with response. Proc Am Soc Clin Oncol. 2012. Abstract 5518. http://meetinglibrary.asco.org/content/100476-114. Accessed March 10, 2015.
- Schlumberger M, Jarzab B, Cabanillas ME, et al. A phase II trial of the multitargeted kinase inhibitor lenvatinib (E7080) in advanced medullary thyroid cancer (MTC). Proc Am Soc Clin Oncol. 2012. Abstract 5591. http://meetinglibrary.asco.org/content/100784-114. Accessed March 10, 2015.
- Vergote I, Teneriello M, Powell MA, et al. A phase II trial of lenvatinib in patients with advanced or recurrent endometrial cancer: Antiopoietin-2 as a predictive marker for clinical outcomes. Proc Am Soc Clin Oncol. 2013. Abstract 5520. http://meetinglibrary.asco.org/content/113008-132. Accessed March 10, 2015.
- O’Day S, Gonzalez R, Kim K, et al. A phase II study of the multitargeted kinase inhibitor lenvatinib in patients with advanced BRAF wild-type melanoma. Proc Am Soc Clin Oncol. 2013. Abstract 9026. http://meetinglibrary.asco.org/content/112958-132. Accessed March 10, 2015.
- Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015 ;372(7):621-630.
- Havel L, Lee JS, Lee KH, et al. E7080 (lenvatinib) in addition to best supportive care (BSC) versus BSC alone in third-line or greater nonsquamous, non-small cell lung cancer (NSCLC). Proc Am Soc Clin Oncol. 2014. Abstract 8043. http://meetinglibrary.asco.org/content/128475-144. Accessed March 10, 2015.
- Mitsunaga S, Ikeda M, Ueno H, et al. Phase I/II study of lenvatinib (E7080), a multitargeted tyrosine kinase inhibitor, in patients (pts) with advanced hepatocellular carcinoma (HCC): Phase I results. Proc Am Soc Clin Oncol. 2013. Abstract 231. http://meetinglibrary.asco.org/content/105252-133. Accessed March 10, 2015.
- Okita K, Kumada H, Ikeda K, et al. Phase I/II study of E7080 (lenvatinib), a multitargeted tyrosine kinase inhibitor, in patients (pts) with advanced hepatocellular carcinoma (HCC): Initial assessment of response rate. Proc Am Soc Clin Oncol. 2012. Abstract 320. http://meetinglibrary.asco.org/content/187667-115. Accessed March 10, 2015.
- Harbour JW, Luo RX, Dei SA, et al. Cdk phosphorylation triggers sequential intramolecular interactions that progressively block Rb functions as cells move through G1. Cell. 1999;98(6):859-869.
- Fry DW, Harvey PJ, Keller PR, et al. Specific inhibition of cyclin-dependent kinase 4/6 by PD 0332991 and associated antitumor activity in human tumor xenografts. Mol Cancer Ther. 2004;3(11):1427-1438.
- Toogood PL, Harvey PJ, Repine JT, et al. Discovery of a potent and selective inhibitor of cyclin-dependent kinase 4/6. J Med Chem. 2005;48(7):2388-2406.
- Schwartz GK, LoRusso PM, Dickson MA, et al. Phase I study of PD 0332991, a cyclin-dependent kinase inhibitor, administered in 3-week cycles (Schedule 2/1). Br J Cancer. 2011;104(12):1862-1868.
- Flaherty KT, Lorusso PM, Demichele A, et al. Phase I, dose-escalation trial of the oral cyclin-dependent kinase 4/6 inhibitor PD 0332991, administered using a 21-day schedule in patients with advanced cancer. Clin Cancer Res. 2012;18(2):568-576.
- Ibrance [prescribing information]. New York: Pfizer Labs; 2015.
- Leonard JP, LaCasce AS, Smith MR, et al. Selective CDK4/6 inhibition with tumor responses by PD0332991 in patients with mantle cell lymphoma. Blood. 2012;119(20):4597-4607.
- Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomized phase 2 study. Lancet Oncol. 2015;16(1):25-35.
- Gopalan PK, Pinder MK, Chiappori A, et al. A phase II clinical trial of the CDK 4/6 inhibitor palbociclib (PD 0332991) in previously treated, advanced non-small cell lung cancer (NSCLC) patients with inactivated CDKN2A. Proc Am Soc Clin Oncol. 2014. Abstract 8077. http://meetinglibrary.asco.org/content/135087-144. Accessed March 10, 2015.
- Mayer EL, Gropper AB, Tung NM, et al. Adjuvant palociclib (P) plus endocrine therapy (ET) for hormone receptor positive (HR+) breast cancer: A phase II feasibility study. Proc Am Soc Clin Oncol. 2014. Abstract TPS654. http://meetinglibrary.asco.org/content/128490-144. Accessed March 10, 2015.
- Littman SJ, Brus C, Burkart A. A phase II study of palociclib (PD-0332991) in adult patients with advanced hepatocellular carcinoma. Proc Am Soc Clin Oncol GI Cancers Symposium. 2015. Abstract 527. http://meetinglibrary.asco.org/content/140466-158. Accessed March 10, 2015.
- O’Hara MH, Edmonds C, Farwell M, et al. Phase II pharmacodynamics trial of palociclib in patients with KRAS mutant colorectal cancer. Proc Am Soc Clin Oncol GI Cancers Symposium. 2015. Abstract 626. http://meetinglibrary.asco.org/content/133702-144. Accessed March 10, 2015.
