ISMP Medication Error Report Analysis
Let’s Target This “Dirty Dozen” for Improvement During 2015
Caution: “Per Liter” Content on Manufacturers’ IV Bag Labels
Michael R. Cohen, RPh, MS, ScD,* and Judy L. Smetzer, RN, BSN†
ISMP Medication Error Report Analysis
Let’s Target This “Dirty Dozen” for Improvement During 2015
Caution: “Per Liter” Content on Manufacturers’ IV Bag Labels
Michael R. Cohen, RPh, MS, ScD,* and Judy L. Smetzer, RN, BSN†
ISMP Medication Error Report Analysis
Let’s Target This “Dirty Dozen” for Improvement During 2015
Caution: “Per Liter” Content on Manufacturers’ IV Bag Labels
Michael R. Cohen, RPh, MS, ScD,* and Judy L. Smetzer, RN, BSN†
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were received through the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers’ names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMP Web site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at ismpinfo@ismp.org. ISMP guarantees the confidentiality and security of the information received and respects reporters’ wishes as to the level of detail included in publications.
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were received through the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers’ names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMP Web site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at ismpinfo@ismp.org. ISMP guarantees the confidentiality and security of the information received and respects reporters’ wishes as to the level of detail included in publications.
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were received through the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers’ names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMP Web site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at ismpinfo@ismp.org. ISMP guarantees the confidentiality and security of the information received and respects reporters’ wishes as to the level of detail included in publications.
Hosp Pharm 2015;50(2):94–98
2015 © Thomas Land Publishers, Inc.
doi: 10.1310/hpj5002-94
LET’S TARGET THIS “DIRTY DOZEN” FOR IMPROVEMENT DURING 2015
As we enter 2015, we are reflecting on the strength and resolve of many across the nation who have demonstrated an unparalleled commitment to keeping patients safe. Despite the many safety accomplishments in 2014, we can’t help but mull over persistent medication safety gaffes that continue unresolved and doggedly test our tenacity. We would like to share our “Dirty Dozen” safety gaffes for the past year with the hope that you will join us in bringing attention to these crucial issues and the compelling need for their resolution.
Changing PhRMA Business Models: Negative Financial Impact on Providers’ Supply Chain Costs
Whether it’s the discontinuation of a low-volume but medically necessary drug leading to critical shortages or increases in the cost of longstanding medications, such as U-500 insulin, when the demand increases, the cost of pharmaceuticals has been highly unpredictable. This has become more of an issue in the last 5 years, wreaking havoc on health care providers’ operational budgets. The latest offense comes from the pharmaceutical giant Genentech. The company has changed its distribution methods for 3 widely used cancer drugs to maximize “business efficiencies” for the company, but the change will result in negative consequences for everyone downstream. Effective October 1, 2014, Avastin (bevacizumab), Herceptin (trastuzumab), and Rituxan (rituximab) are only being shipped to health care providers via 6 authorized specialty distributors instead of the usual wholesalers. Genentech’s choice to not contract for cost relief on any of its products means that hospitals will now lose any prior cost savings based on wholesaler contracts and will frequently incur higher costs to manage their drug distribution process, requiring more products in stock and less just-in-time ordering. For a large cancer center, the change will add $1 million or more annually in pharmaceutical costs with little advanced warning, reducing the dollars available to provide care to patients. While the Department of Health and Human Services (HHS) is trying to contain the costs of health care on the provider end, there seems to be little effort to contain costs on the supply end. The budgets needed for pharmaceuticals that are crucial to patient care appear to be increasing at the financial whim of big pharmaceutical companies.
Clear Care: Still Causing Severe Eye Injuries
Since early 2010, ISMP has received scores of reports of painful eye injuries from patients using Clear Care cleaning and disinfecting solution for contact lenses, by Alcon (formerly CIBA VISION), a Novartis company. Hundreds more can be found on Internet listservs. Located on store shelves near other lens disinfectants and solutions, Clear Care differs from other commonly used solutions in that it must be used with a special lens case to neutralize the 3% hydrogen peroxide component of the solution over at least 6 hours before putting the lenses back into the eyes. However, many have used the solution inadvertently to soak their lenses in a standard lens case or thought the solution was saline and instilled it directly into their eyes. This has caused severe eye burning, which has led many users to seek out emergency medical care for corneal burns. In 2012, the company made a minor label enhancement to warn customers to use the special lens case, but the label change has been ineffective. Neither the company nor the US Food and Drug Administration’s (FDA) device division have been persuaded to make effective label improvements before permanent eye injury or blindness occurs. If the labeling and packaging cannot be improved to reduce the harm being reported, perhaps this dangerous product should be pulled from the market or available only behind the pharmacy counter.
Patient Counseling: Only a Veiled “Offer” in Many States
The effectiveness of patient counseling in a community pharmacy to detect and prevent medication errors, and its link to improved medication adherence and positive clinical outcomes, have been well documented in the literature. Yet, studies have placed patient counseling rates at only 8% to 42%. An increase in the frequency and quality of patient counseling has been linked to state-specific regulations that require patient counseling for new prescriptions coupled with strict enforcement surveillance. States that require an “offer” to counsel have very low patient counseling rates. Patients often fail to recognize an offer to counsel when simply asked, “Do you have any questions?” or told to “Sign here.” They may not even know what to ask. This means that, with few exceptions, pharmacies in states that require only an offer to counsel will likely dispense a powerful opioid such as fentanyl patches, for example, and allow the patient or caregiver to walk out of the pharmacy without so much as a brief discussion about safe use and disposal. ISMP has long promoted mandatory patient counseling in community pharmacies for targeted high-alert medications, with less emphasis on current ineffective regulations that require an “offer” to counsel for all medications.
Patients Impacted by Dispensing Errors: Callous Response from Pharmacists
When patients report dispensing errors to ISMP, they are usually more upset about the response they received when contacting the pharmacist or pharmacy manager than the actual error itself. All too often, consumers tell us that pharmacy staff have responded in a callous manner when confronted with the possibility of a dispensing error, demonstrating a lack of empathy and concern for the adverse effects the patient might have experienced. The patients are often asked to return the erroneous medication to the pharmacy (relinquishing key evidence if legal remedy is sought) and then given the correct medication. Some pharmacies also offer a $25 discount coupon or refund for the cost of the erroneous prescription, but a signature may be required to document that the patient has accepted the coupon or refund as full restitution of the mistake. Although pharmacy staff may want to be more responsive to patients who report errors, they are often following corporate policies that are focused on legal concerns. As patients are continually encouraged to be active participants in their health care, they want and deserve honest disclosure of errors and knowledge that there’s an action plan to reduce the risk of it happening again.
Manufacturers’ Prefilled Syringes: Misuse Spanning at Least 7 Years
Based on surveys, observations, and error reports, ISMP is aware that many practitioners misuse prefilled syringes in a manner that renders them unsafe. First, the prefilled drug cartridges are often used as single- or multiple-dose vials by removing all or part of the contents through the rubber diaphragm or the small hole at the top of the needleless system connector. However, the cartridge is not intended for puncture, and the contents do not include preservatives or antimicrobial agents; thus, the risk of contamination is high, and measurement errors are also possible. While the prefilled cartridges include a barcode, the final practitioner-prepared syringes do not and are rarely labeled. Practitioners have also misused prefilled syringes of saline flushes when drawing a drug into the saline flush syringe to dilute the medication or when the saline is used to reconstitute a lyophilized powder and then drawn back into the saline flush syringe. This dangerous practice leads to a syringe being labeled as saline but actually containing both saline and the drug. In 2007, one company that makes saline flushes had widened the gradations on the syringes to discourage this practice, as more precise gradations are usually needed to measure doses accurately. Unfortunately, this measure has not stopped the practice. Single-dose vials of saline or sterile water for injection must be provided and used if drugs require reconstitution or dilution in a patient care area.
Syringe Pull-Back Method for Verifying IV Admixtures: Overreliance on a Weak Strategy
Many hospital IV admixture processes rely on the syringe pull-back method as the method the pharmacist uses to check the admixture and assess how much medication or diluent was added to the infusion container. The empty syringe is accompanied by the actual drug or diluent container displayed next to the syringe. For years, ISMP has discouraged reliance on this method, particularly for chemotherapy, complex electrolyte solutions, or compounded sterile products with other high-alert medications. The method, now prohibited by some state boards of pharmacy, is prone to errors when the user pulls back the plunger to the volume of product he or she believes was included in the admixture and when the syringes are placed near the corresponding vials. Also, for the person checking the products, it may not be clear which syringe goes with which vial. This method of verification is weak in comparison to manual or automated checking of the products and volumes in syringes before addition to the admixture container.
Compounded Pain Creams: High Profit Margin and Danger
Some compounding pharmacies have been heavily marketing compounded pain creams directly to consumers via unsolicited calls, suggesting that the creams are more effective and safer than oral or injectable pain medications. Many of the creams contain drugs that can cause central nervous system depression or adverse cardiac effects, and most have not been FDA-approved for use in combination with each other or for topical use. Patients are charged per ingredient, with many creams containing numerous, expensive medications. Toxicity from the creams has been reported to poison control centers, including cases of accidental child exposures and intentional use for multiple family members. Patients are often unaware of the dangers with using the creams, including unsafe packaging in containers without child-resistant closures. We are specifically concerned about some statements that may be unproven, such as the products’ safe use with children. Compounded pain creams need prominent warnings on labels that describe the potential for toxicity, and physicians and pharmacists who prescribe and dispense the creams must provide patients with instructions about possible adverse effects, safe storage, and proper use. We believe regulatory or licensing oversight is necessary.
Disrespectful Behavior: A History of Tolerance in Health Care
Bullying, incivility, and other forms of disrespectful behavior are still rampant in health care, and we allow this when we tolerate the behavior, remain silent, or make excuses in an attempt to minimize the profound devastation that disrespectful behavior causes. An ISMP survey conducted in 2003 clearly demonstrated the scope of disrespectful behavior among many levels of interdisciplinary staff, and an ISMP survey a decade later demonstrated little improvement. Our slow progress is not due to lack of resources or know-how but to a dysfunctional culture, with a central ethos that favors a sense of privilege, status, and autonomy, thus impairing teamwork and communication. Disrespect diminishes a person’s ability to think clearly, make sound judgments, speak up regarding questions, or avoid at-risk behaviors. Disrespectful behaviors also underlie a resistance to collaborate with others, follow procedures that promote safe practices, or implement new safety practices. Whereas a culture of disrespect is harmful on many levels, its effect on patient safety makes it a matter of national urgency.
Independent Double-Checks: Undervalued and Misused
Manual independent double-checks of high-alert medications is a strategy that has been widely promoted to help detect potentially harmful errors before they reach patients. However, their value has been disputed, and their use has been a source of stress for busy prescribers, pharmacists, and nurses who are short on time. Their impact on safety has been questioned by those who rarely find mistakes during the checking process. Their inconsistent use, variability in how the task is carried out, and overuse for all high-alert medications has rendered them incapable of detecting many errors. Failed checking processes can often be traced to: auto-processing in which the person checking the work does so in a habitual manner with little real appraisal; deference to authority in which the person is checking the work of someone who outranks him or her; reduction of responsibility in which staff believe someone else will catch any mistakes; and lack of time. What is often missing in the double-check process is a more cognitive review of all components of the medication, beyond verification of the “5 rights,” that requires purposeful thought. Additionally, independent double-checks must be strategically placed for just a few select high-alert medications, and they should never serve as the only safety net in place to prevent or detect errors with these medications.
Beyond-Use Dating of Drugs: CMS Standards Lead to Costly Waste
To avoid the use of outdated drugs, the Centers for Medicare & Medicaid Services (CMS) requires pharmacists to follow the manufacturer’s directions regarding storage, stability, and beyond-use dating in the official FDA-approved prescribing information. The Joint Commission (TJC) and other accrediting organizations follow guidance from the CMS on this issue. However, this has proven difficult and wasteful—especially in cases of critical drug shortages—for 2 primary reasons: (1) complete information on storage, stability, compatibility, and beyond-use dating is often not provided in the official prescribing information, and (2) newer, evidence-based information on these matters can sometimes be found in peer-reviewed scientific journals and compendia fully endorsed by national pharmacy organizations. If information on storage, stability, and beyond-use dating is not available in the manufacturer’s directions, CMS and accrediting agencies defer to recommendations available in nationally recognized sources. ISMP and the American Society of Health-System Pharmacists (ASHP) have brought the issue to the CMS, but the government agency is confronted with a dilemma if the official, FDA-approved manufacturer’s directions differ from newer, evidence-based recommendations in national compendia. The CMS has been reviewing this matter since 2012. However, surveyors from the CMS and accrediting agencies are still citing organizations for not following the explicit directions in the manufacturer’s package insert despite newer, reliable evidence, unless they have a letter of support from the manufacturer.
Vaccine Errors: Repetitive Errors Reported in the Last Decade
How many DTaP (diphtheria and tetanus toxoids, and acellular pertussis) and Tdap (tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis) vaccine mix-ups need to occur before regulatory action is taken to prevent confusion? Whatever the number, we can say that we have probably met that threshold! Yet, vaccine errors like this continue to occur at an alarming rate (based on those reported to ISMP alone). Vaccine mix-ups often occur due to age-dependent formulations of the same vaccine, similar vaccine abbreviations, similar vaccine containers and labels, and storage near each other. Confusion between the diluent and vaccine has led to administration of the diluent alone or use of the wrong diluent (which happened in Syria last September, causing the death of 15 children). With an unfortunate rise in parents choosing not to vaccinate their children or themselves, we cannot continue to make errors when vaccinating those who choose to be immunized. The impact of inaction on both individual and community immunity may be far-reaching.
Wrong Patient Errors: Not Opening the Bag at the Point of Sale
Community pharmacies are vulnerable to dispensing correctly filled prescriptions to the wrong patient (or family member, friend, or caregiver) at the point of sale, a risk that is well substantiated in the literature. This error is not influenced by the attributes of a specific medication; thus, dispensing any prescription medication to the wrong patient at the point of sale carries a similar level of risk. Based on an ISMP study, the error happens at an estimated rate of 1.22 per 1,000 prescriptions. Among approximately 56,000 community pharmacies in the United States, this error rate suggests that 332,755 prescriptions will be dispensed to the wrong patient each month, or about 6 every month per pharmacy. One of the most effective ways to prevent this error is to open the bag of filled prescriptions at the point of sale to verify that the drugs are for the correct patient. With this simple step, the risk of error is reduced by 56%, according to the ISMP study. Yet, few pharmacies follow this practice.
CAUTION: “PER LITER” CONTENT ON MANUFACTURERS’ IV BAG LABELS
A pharmacy ran out of 3% sodium chloride and had to prepare the product using an automated IV compounder. The product formula was entered into the compounding software and double checked by the pharmacy manager and the informatics pharmacist. Still, a mathematical error resulted in a 6% product that was labeled as a 3% product; thus, a review of the error was conducted.
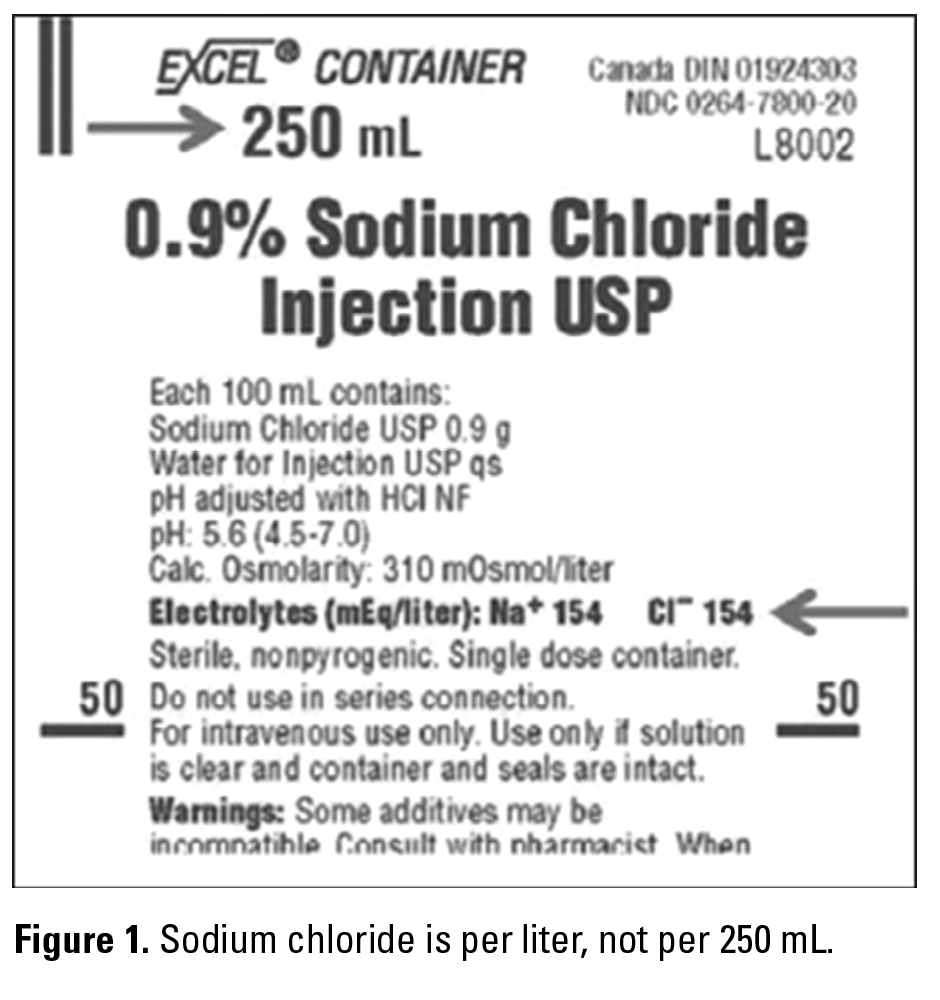
One thing both pharmacists mentioned was the way electrolyte concentrations are listed on IV bags. Concentrations are listed per 1,000 mL, not per container volume. For example, a 250 mL 0.9% sodium chloride injection container label lists the sodium chloride content as 154 mEq/1,000 mL rather than 38.5 mEq/250 mL (see Figure 1).
To make a 500 mL bag of 3% sodium chloride, the pharmacists mistakenly set the proportion up as 154/0.9 = x/3 and came up with the number of mEq needed, 513 mEq of sodium chloride. However, they actually needed only 256-257 mEq of sodium chloride for the 500 mL bag. After several bags had been dispensed, a third pharmacist identified the error when checking a finished bag along with the used sodium chloride concentrate container. Several patients were potentially exposed to the error. All providers were notified, and the sodium level was monitored for patients at risk. The patients, who were being treated for hyponatremia or increased intracranial pressure, were not harmed.
The pharmacy is now determined to avoid adding standard formulas to the automated IV compounder “on the fly.” Instead, prior to becoming an emergent/urgent need, they plan to preprogram formulas when solutions are at risk for drug shortages. They also plan to increase communication with their supplier to make every effort to keep commercial products available. The way the concentration is listed on IV bags has tripped up many pharmacists and nurses over the years. It’s time for the FDA and the US Pharmacopeial Convention (USP) to rethink this with large volume parenterals (LVPs). For single- and multiple-dose injectables, USP requires strength per total volume as the primary, prominent display on the label, followed in close proximity by strength per mL enclosed in parentheses. We think this should apply to LVPs as well.![]()
*President, Institute for Safe Medication Practices, 200 Lakeside Drive, Suite 200, Horsham, PA 19044; phone: 215-947-7797; fax: 215-914-1492; e-mail: mcohen@ismp.org; Web site: www.ismp.org. †Vice President, Institute for Safe Medication Practices, Horsham, Pennsylvania.