Endoscopic Management of Bladder Diverticula
Khanh N. Pham, MD, Claudio Jeldres, MD, Thomas Hefty, MD, John M. Corman, MD
Section of Urology and Renal Transplantation, Virginia Mason Hospital and Medical Center, Seattle, WA
A 50-year-old man with benign prostatic hyperplasia and urinary retention had a very large diverticulum on the posterior wall of the bladder. The patient was managed with transurethral resection of the prostate and endoscopic fulguration of the bladder diverticulum mucosa using the Orandi technique. There was near-complete resolution of the bladder diverticulum following endoscopic management, obviating the need for bladder diverticulectomy. The patient now empties his bladder, with a postvoid residual < 50 mL and the absence of urinary tract infection after 6-month follow-up. We report the successful treatment of a large bladder diverticulum with endoscopic fulguration to near-complete resolution. This minimally invasive technique is a useful alternative in patients unfit for a more extensive surgical approach.
[Rev Urol. 2016;18(2):114-117 doi: 10.3909/riu0701]
© 2016 MedReviews®, LLC
Endoscopic Management of Bladder Diverticula
Khanh N. Pham, MD, Claudio Jeldres, MD, Thomas Hefty, MD, John M. Corman, MD
Section of Urology and Renal Transplantation, Virginia Mason Hospital and Medical Center, Seattle, WA
A 50-year-old man with benign prostatic hyperplasia and urinary retention had a very large diverticulum on the posterior wall of the bladder. The patient was managed with transurethral resection of the prostate and endoscopic fulguration of the bladder diverticulum mucosa using the Orandi technique. There was near-complete resolution of the bladder diverticulum following endoscopic management, obviating the need for bladder diverticulectomy. The patient now empties his bladder, with a postvoid residual < 50 mL and the absence of urinary tract infection after 6-month follow-up. We report the successful treatment of a large bladder diverticulum with endoscopic fulguration to near-complete resolution. This minimally invasive technique is a useful alternative in patients unfit for a more extensive surgical approach.
[Rev Urol. 2016;18(2):114-117 doi: 10.3909/riu0701]
© 2016 MedReviews®, LLC
Endoscopic Management of Bladder Diverticula
Khanh N. Pham, MD, Claudio Jeldres, MD, Thomas Hefty, MD, John M. Corman, MD
Section of Urology and Renal Transplantation, Virginia Mason Hospital and Medical Center, Seattle, WA
A 50-year-old man with benign prostatic hyperplasia and urinary retention had a very large diverticulum on the posterior wall of the bladder. The patient was managed with transurethral resection of the prostate and endoscopic fulguration of the bladder diverticulum mucosa using the Orandi technique. There was near-complete resolution of the bladder diverticulum following endoscopic management, obviating the need for bladder diverticulectomy. The patient now empties his bladder, with a postvoid residual < 50 mL and the absence of urinary tract infection after 6-month follow-up. We report the successful treatment of a large bladder diverticulum with endoscopic fulguration to near-complete resolution. This minimally invasive technique is a useful alternative in patients unfit for a more extensive surgical approach.
[Rev Urol. 2016;18(2):114-117 doi: 10.3909/riu0701]
© 2016 MedReviews®, LLC
Key words
Bladder diverticulum • Endoscopic • Fulguration
Key words
Bladder diverticulum • Endoscopic • Fulguration
Cystoscopic evaluation demonstrated a large bladder diverticulum with a moderately sized neck that was located on the posterior aspect of the bladder.
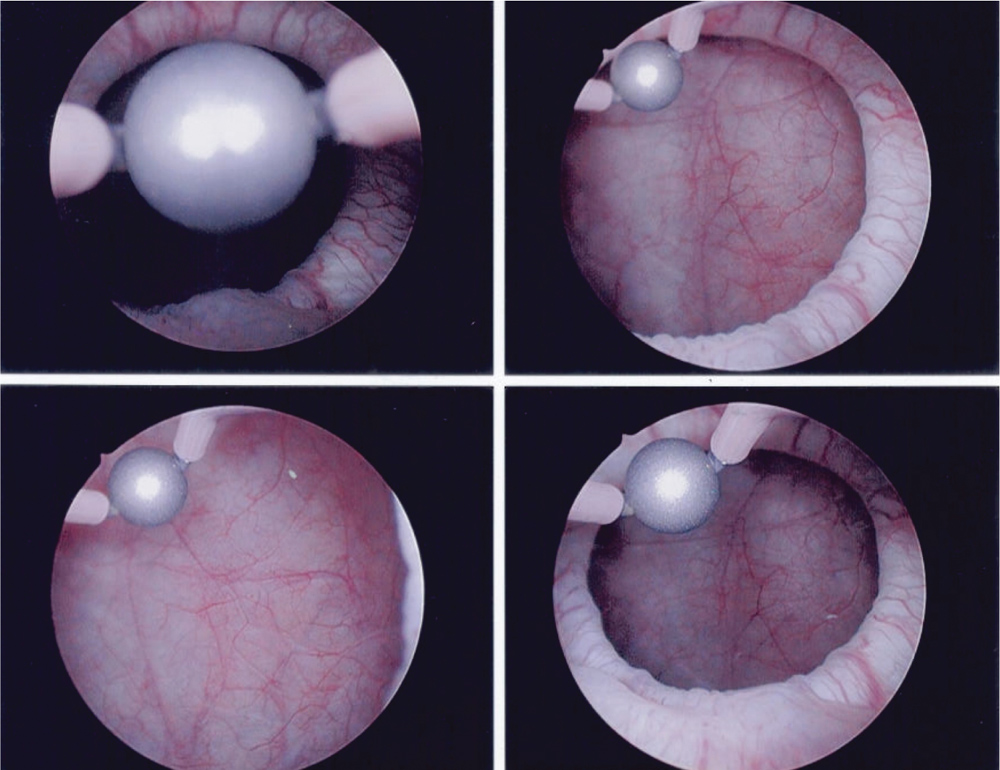
Figure 1. Cystoscopic images of the bladder before therapy.
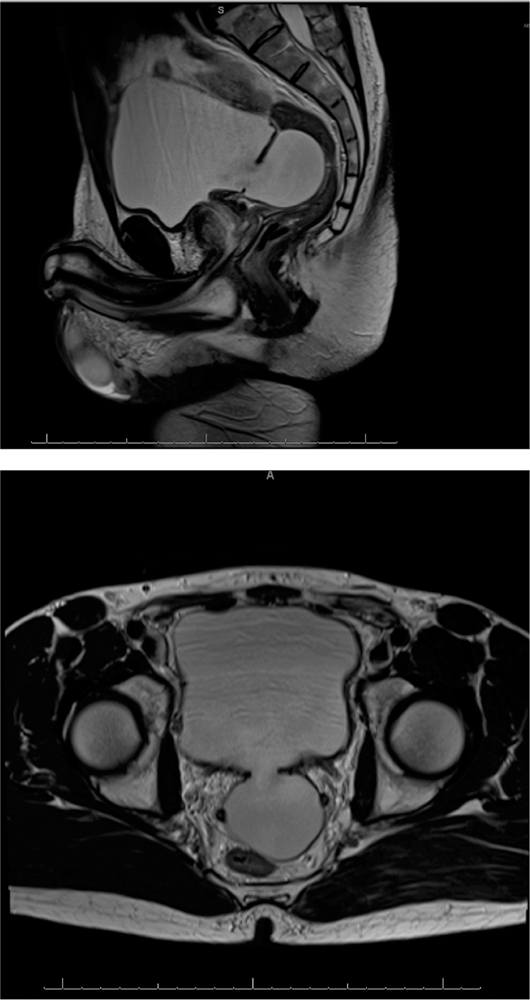
Figure 2. Magnetic resonance images of the bladder diverticulum before therapy.
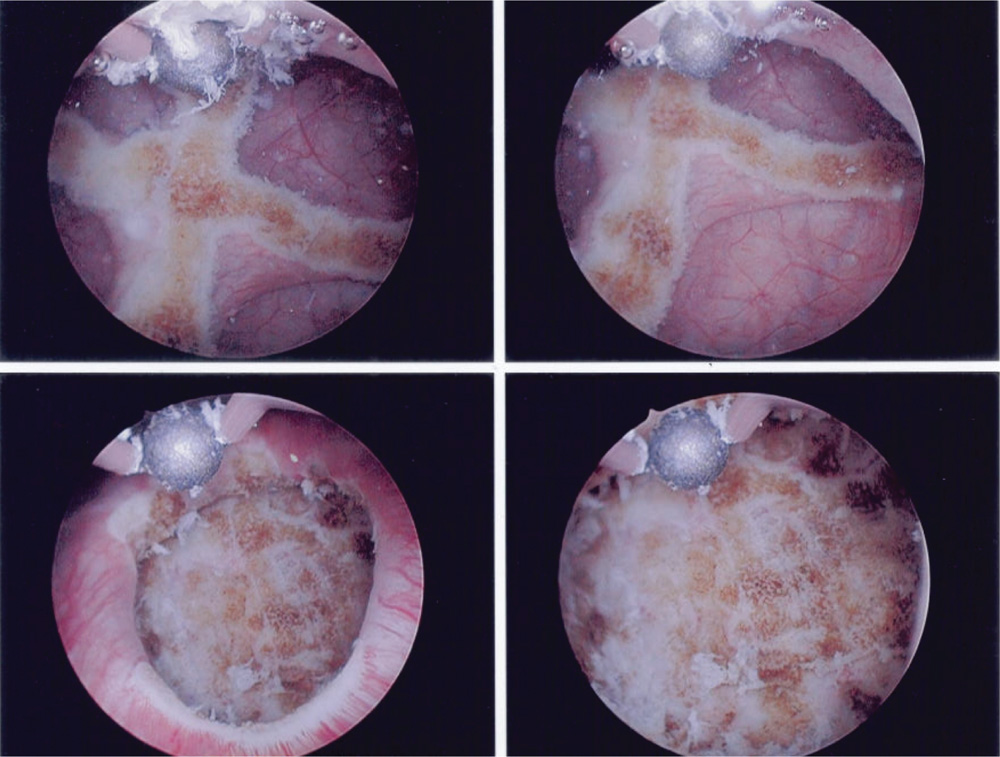
Figure 3. Cystoscopic images showing the urothelial lining of the entire bladder diverticulum after therapy.
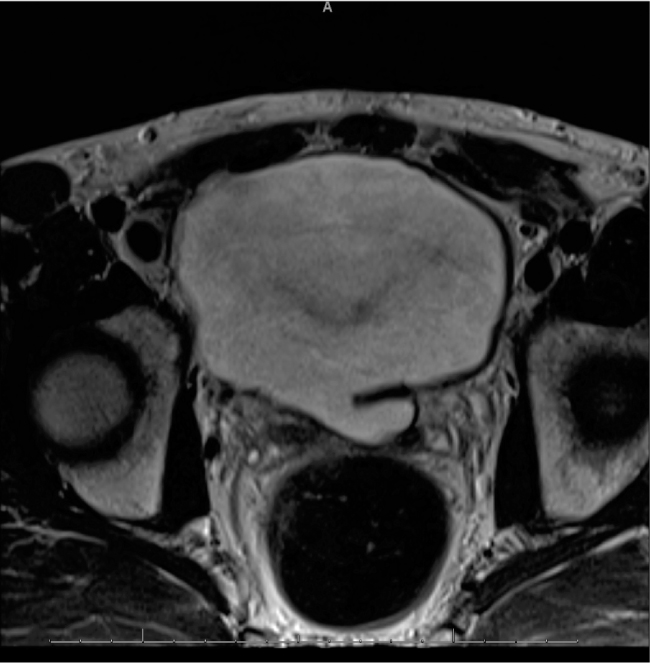
Figure 4. Magnetic resonance images of the bladder diverticulum after therapy.
Main Points
• Bladder diverticula in adult men typically occur in the setting of bladder outlet obstruction. Although many bladder diverticula are asymptomatic, they can be incidentally discovered on evaluation for hematuria, bladder outlet obstruction, or urinary tract infection.
• Bladder diverticula can be managed in several different ways, including conservative nonoperative management, surgical excision, and endoscopic management. Indications for treating bladder diverticula include urinary infection, stones, or malignancy.
• This report describes the first modern-era report of endoscopic fulguration of a bladder diverticulum to near-complete resolution. The technique was successful in achieving a favorable outcome in a minimally invasive fashion.
• We advocate consideration of endoscopic fulguration of bladder diverticula in patients who may be unfit for surgery, such as older patients with multiple comorbidities, patients with previous abdominal surgery or radiation, and patients on anticoagulation therapy.
Main Points
• Bladder diverticula in adult men typically occur in the setting of bladder outlet obstruction. Although many bladder diverticula are asymptomatic, they can be incidentally discovered on evaluation for hematuria, bladder outlet obstruction, or urinary tract infection.
• Bladder diverticula can be managed in several different ways, including conservative nonoperative management, surgical excision, and endoscopic management. Indications for treating bladder diverticula include urinary infection, stones, or malignancy.
• This report describes the first modern-era report of endoscopic fulguration of a bladder diverticulum to near-complete resolution. The technique was successful in achieving a favorable outcome in a minimally invasive fashion.
• We advocate consideration of endoscopic fulguration of bladder diverticula in patients who may be unfit for surgery, such as older patients with multiple comorbidities, patients with previous abdominal surgery or radiation, and patients on anticoagulation therapy.
Bladder diverticula in adult men typically occur in the setting of bladder outlet obstruction. The prevalence of bladder diverticula in association with benign prostatic hyperplasia (BPH) is approximately 6%.1 Although many bladder diverticula are asymptomatic, they can be incidentally discovered on evaluation for hematuria, bladder outlet obstruction, or urinary tract infection.
Chronic urinary stasis within bladder diverticula can result in bladder calculi and subsequent infections. Additionally, concerns regarding malignant transformation exist, highlighting the importance of appropriate management. A variety of management options exist, including formal diverticulectomy either by open or laparoscopic approach. Endoscopic options have also been reported, including transurethral resection of the diverticular neck and fulguration of the urothelial mucosa of the diverticulum.2-5 Although the technique was first described by Orandi in 1977,5 most related reports predate modern day urodynamic and imaging techniques. This report describes the use of endoscopic fulguration of a large bladder diverticulum to near resolution in a modern clinical setting.
Case Report
A 50-year-old man was evaluated for lower urinary tract voiding symptoms and found to have BPH with urinary retention and a postvoid residual (PVR) > 500 mL. Cystoscopic evaluation demonstrated a large bladder diverticulum with a moderately sized neck that was located on the posterior aspect of the bladder (Figure 1). Magnetic resonance imaging (MRI) also demonstrated the bladder diverticulum posteriorly in the midline (Figure 2).
The patient was offered minimally invasive management of his BPH with transurethral resection of the prostate and endoscopic fulguration of the bladder diverticulum with a cystoscopic roller ball. The urothelial lining of the entire bladder diverticulum, as well as the mucosa beyond the diverticular neck, was fulgurated using electrocoagulation (Figure 3). MRI following endoscopic management demonstrated near-complete resolution of the bladder diverticulum (Figure 4).
Urodynamic studies were performed following the procedure. The patient had normal sensation to void. The maximum flow rate was 11.5 mL/sec, with an average flow rate of 6.2 mL/sec. There was a PVR volume of 50 mL after a voided volume of 250 mL.
Discussion
Bladder diverticula are typically classified as either congenital or acquired. Acquired bladder diverticula develop due to bladder outlet obstruction or neurogenic bladder. Most bladder diverticula are asymptomatic and are commonly discovered during investigation for hematuria, lower urinary tract symptoms, or infection. Some can also be found incidentally upon radiographic imaging.6
Bladder diverticula can be managed in several different ways, including conservative nonoperative management, surgical excision, and endoscopic management. Indications for treating bladder diverticula include urinary infection, stones, or malignancy. Malignancy can be of particular concern with regard to bladder diverticula due to the lack of a muscular wall beyond the mucosal layer, potentially resulting in increased risk for extension of possible malignancy outside the bladder.2 Open bladder diverticulectomy is the most invasive management modality and can be performed by either a transvesical or extravesical approach.7
Several reports in the literature have described the use of endoscopic management of bladder diverticula using transurethral endoscopic fulguration of the bladder diverticula mucosa and/or incision of the urinary bladder’s diverticular neck. Orandi5 first published a report on a series of 17 patients who underwent transurethral fulguration, demonstrating complete resolution in 5 patients and a decrease in size in 9 patients on cystograms obtained from 1 week to 12 months after surgery. Clayman and colleagues similarly managed six patients with transurethral fulguration, five of whom had no diverticula seen on follow-up cystogram and one who had a notable decrease in volume.2 In 1992, Yamaguchi and colleagues3 reported the most recent and largest series to date utilizing endoscopic management of bladder diverticula by transurethral resection of the diverticular neck and fulguration of the diverticular mucosa in 31 diverticula. Cystograms performed 1 month after surgery demonstrated complete resolution in 26 diverticula with a decrease in volume in the remaining 5 diverticula of 60% to 99%.
We describe the first modern-era report of endoscopic fulguration of a bladder diverticulum to near-complete resolution. Although the patient in this report did not have significant comorbidities precluding him from an open diverticulectomy, this technique was successful in achieving a favorable outcome in a minimally invasive fashion. We advocate consideration of endoscopic fulguration of bladder diverticula in patients who may be unfit for surgery, such as older patients with multiple comorbidities, patients with previous abdominal surgery or radiation, and patients on anticoagulation therapy. This approach offers favorable outcomes and its use has been supported over several decades. This case adds to the literature in that now, more than 20 years after the most recent report, we have clear, high-quality intraoperative images demonstrating the technique, as well as excellent radiographic images both before and after surgery. ![]()
References
- Burns E. Diverticula of the urinary bladder. Ann Surg. 1944;119:656-664.
- Clayman RV, Shahin S, Reddy P, Fraley EE. Transurethral treatment of bladder diverticula. Alternative to open diverticulectomy. Urology. 1984;23:573-577.
- Yamaguchi K, Kotake T, Nishikawa Y, et al. Transurethral treatment of bladder diverticulum. Urol Int. 1992;48:210-212.
- Adachi M, Nakada T, Suzuki H, et al. Successful repair of huge bladder diverticulum with a transurethral fulguration. Report of a case. Urol Int. 1991;46:87-89.
- Orandi A. Transurethral fulguration of bladder diverticulum: new procedure. Urology. 1977;10:30-32.
- Rovner, ES. Bladder and female urethral diverticula. In: McDougal S, ed. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Elsevier Saunders; 2012: 2262-2271.
- Gil-Vernet JM. Bladder diverticulectomy. In: Graham SD, ed. Glenn’s Urologic Surgery. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1998: 205-209.