How Would You Manage?
Raoul S. Concepcion, MD, FACS
Urology Associates, Nashville, Nashville, TN
[Rev Urol. 2016;18(1):44-45 doi: 10.3909/riu0709]
© 2016 MedReviews®, LLC
How Would You Manage?
Raoul S. Concepcion, MD, FACS
Urology Associates, Nashville, Nashville, TN
[Rev Urol. 2016;18(1):44-45 doi: 10.3909/riu0709]
© 2016 MedReviews®, LLC
How Would You Manage?
Raoul S. Concepcion, MD, FACS
Urology Associates, Nashville, Nashville, TN
[Rev Urol. 2016;18(1):44-45 doi: 10.3909/riu0709]
© 2016 MedReviews®, LLC
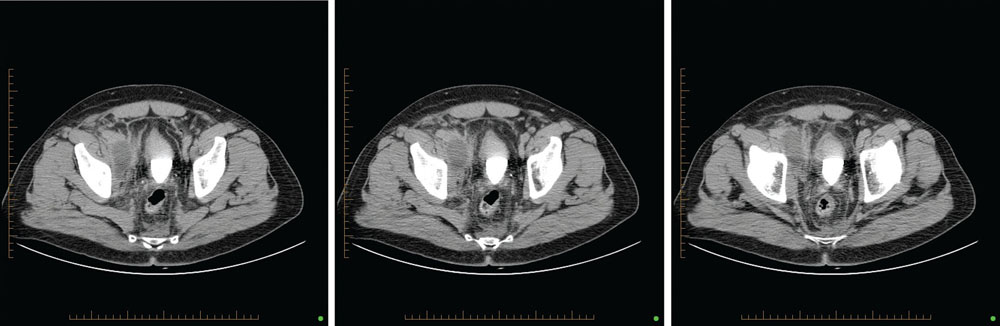
Figure 1. Computed tomography of abdomen and pelvis, with and without intravenous contrast (April 24, 2012).
Figure 1. Computed tomography of abdomen and pelvis, with and without intravenous contrast (April 24, 2012).
In the early to mid-1990s, a cardiovascular surgeon (a colleague and friend) told me that the most beneficial meeting he attended annually was a 2-day conference at which attendees presented actual cases and complications, about which the audience then opined on management. In this edition of Reviews in Urology, we are debuting a new section entitled How Would You Manage? A brief clinical vignette is presented with an associated unplanned outcome/event. Appropriate images are included, followed by a series of multiple-choice questions that we would like you, the readers, to answer. The results will be tabulated and made available in the subsequent edition, along with the actual management of the case by the submitting physician. We want your opinions on this format, both positive and negative, and suggestions on ways to improve upon its design. The Editorial Board also encourages readers to submit their own personal cases.
Case Details
WM, a 54-year-old man, referred for a sudden rise in prostate-specific antigen (PSA) level to 11.57 ng/mL. Healthy, no family history of prostate cancer, no voiding symptoms, sexually active. No suspicious lesions on digital rectal examination. Biopsy recommended.
January 21, 2012: Transrectal ultrasonography of the prostate/sextant needle biopsy. Prostate volume: 30.3 g, PSA density: 0.38.
3/12 cores (+)
Right base: Gleason 3 + 4, 10%
Right mid: Gleason 3 + 4, 20%
Right apex: Gleason 3 + 3, 10%
March 6, 2012: Robotically assisted prostatectomy, bilateral node dissection. Estimated blood loss: 75 mL.
Final path: pT3c (+ right seminal vesicle), N0, M0, bilateral disease, 45% of gland. Discharge on postoperative day 1, catheter left in place for 7 days.
April 19, 2012: PSA < 0.008 ng/ mL, mild urge incontinence.
April 24, 2012: Patient complains of low-grade fever, “tingling to top of head,” right hip pain with walking.
Laboratory results: leukocyte count 11,400, hemoglobin and hematocrit count 15g/dL/43.6%, urinalysis 0 leukocytes/erythrocytes
Computed tomography (CT) of abdomen and pelvis, with and without intravenous contrast, shown below.
How Would You Manage?
What is your working diagnosis?
A. Resolving hematoma
B. Lymphocele
C. Urinoma
D. Hematocele
E. Diverticular abscess
Do you obtain further imaging studies?
A. Yes
B. No
What are your next steps for management?
A. Needle aspiration of fluid mass under CT guidance
B. Placement of percutaneous drain under CT guidance with intravenous antibiotic therapy
C. Intravenous antibiotic therapy only
D. Open surgical drainage
E. Laparoscopic drainage/marsupialization
