Management of Vesicoureteral Reflux by Endoscopic Injection of Dextranomer/Hyaluronic Acid in Adults
Timothy W. Stark, MD,1 John M. Lacy, MD,2 David M. Preston, MD2,3
1University of Kentucky College of Medicine, and Department of Urology, University of Kentucky, Lexington, KY;2Department of Urology, University of Kentucky College of Medicine, Lexington, KY;3Division of Urology, Veterans Affairs Medical Center, Cooper Drive Division, Lexington, KY
A 74-year-old man presented for evaluation after discovery of a left bladder-wall tumor. He underwent transurethral resection of bladder tumor (TURBT) operation for treatment of low-grade, Ta urothelial cancer of the bladder. The patient developed recurrent disease and returned to the operating room for repeat TURBT, circumcision, and administration of intravesical mitomycin C. The patient developed balanitis xerotica obliterans 4 years post-circumcision, requiring self-dilation with a catheter. He subsequently developed 3 consecutive episodes of left-sided pyelonephritis. Further investigation with voiding cystourethrogram (VCUG) revealed Grade 3, left-sided vesicoureteral reflux (VUR). Due to existing comorbidities, the patient elected treatment with endoscopic dextranomer/hyaluronic acid injection. A post-operative VCUG demonstrated complete resolution of left-sided VUR. This patient has remained symptom free for 8 months post-injection, with no episodes of pyelonephritis.
[Rev Urol. 2016;18(1):46-50 doi: 10.3909/riu0689]
© 2016 MedReviews®, LLC
Management of Vesicoureteral Reflux by Endoscopic Injection of Dextranomer/Hyaluronic Acid in Adults
Timothy W. Stark, MD,1 John M. Lacy, MD,2 David M. Preston, MD2,3
1University of Kentucky College of Medicine, and Department of Urology, University of Kentucky, Lexington, KY;2Department of Urology, University of Kentucky College of Medicine, Lexington, KY;3Division of Urology, Veterans Affairs Medical Center, Cooper Drive Division, Lexington, KY
A 74-year-old man presented for evaluation after discovery of a left bladder-wall tumor. He underwent transurethral resection of bladder tumor (TURBT) operation for treatment of low-grade, Ta urothelial cancer of the bladder. The patient developed recurrent disease and returned to the operating room for repeat TURBT, circumcision, and administration of intravesical mitomycin C. The patient developed balanitis xerotica obliterans 4 years post-circumcision, requiring self-dilation with a catheter. He subsequently developed 3 consecutive episodes of left-sided pyelonephritis. Further investigation with voiding cystourethrogram (VCUG) revealed Grade 3, left-sided vesicoureteral reflux (VUR). Due to existing comorbidities, the patient elected treatment with endoscopic dextranomer/hyaluronic acid injection. A post-operative VCUG demonstrated complete resolution of left-sided VUR. This patient has remained symptom free for 8 months post-injection, with no episodes of pyelonephritis.
[Rev Urol. 2016;18(1):46-50 doi: 10.3909/riu0689]
© 2016 MedReviews®, LLC
Management of Vesicoureteral Reflux by Endoscopic Injection of Dextranomer/Hyaluronic Acid in Adults
Timothy W. Stark, MD,1 John M. Lacy, MD,2 David M. Preston, MD2,3
1University of Kentucky College of Medicine, and Department of Urology, University of Kentucky, Lexington, KY;2Department of Urology, University of Kentucky College of Medicine, Lexington, KY;3Division of Urology, Veterans Affairs Medical Center, Cooper Drive Division, Lexington, KY
A 74-year-old man presented for evaluation after discovery of a left bladder-wall tumor. He underwent transurethral resection of bladder tumor (TURBT) operation for treatment of low-grade, Ta urothelial cancer of the bladder. The patient developed recurrent disease and returned to the operating room for repeat TURBT, circumcision, and administration of intravesical mitomycin C. The patient developed balanitis xerotica obliterans 4 years post-circumcision, requiring self-dilation with a catheter. He subsequently developed 3 consecutive episodes of left-sided pyelonephritis. Further investigation with voiding cystourethrogram (VCUG) revealed Grade 3, left-sided vesicoureteral reflux (VUR). Due to existing comorbidities, the patient elected treatment with endoscopic dextranomer/hyaluronic acid injection. A post-operative VCUG demonstrated complete resolution of left-sided VUR. This patient has remained symptom free for 8 months post-injection, with no episodes of pyelonephritis.
[Rev Urol. 2016;18(1):46-50 doi: 10.3909/riu0689]
© 2016 MedReviews®, LLC
Key words
Dextranomer/hyaluronic acid • Vesicoureteral reflux • Pyelonephritis
Key words
Dextranomer/hyaluronic acid • Vesicoureteral reflux • Pyelonephritis

Figure 1. Pretreatment voiding cystourethrogram demonstrating left vesicoureteral reflux into the lower ureteral segment.
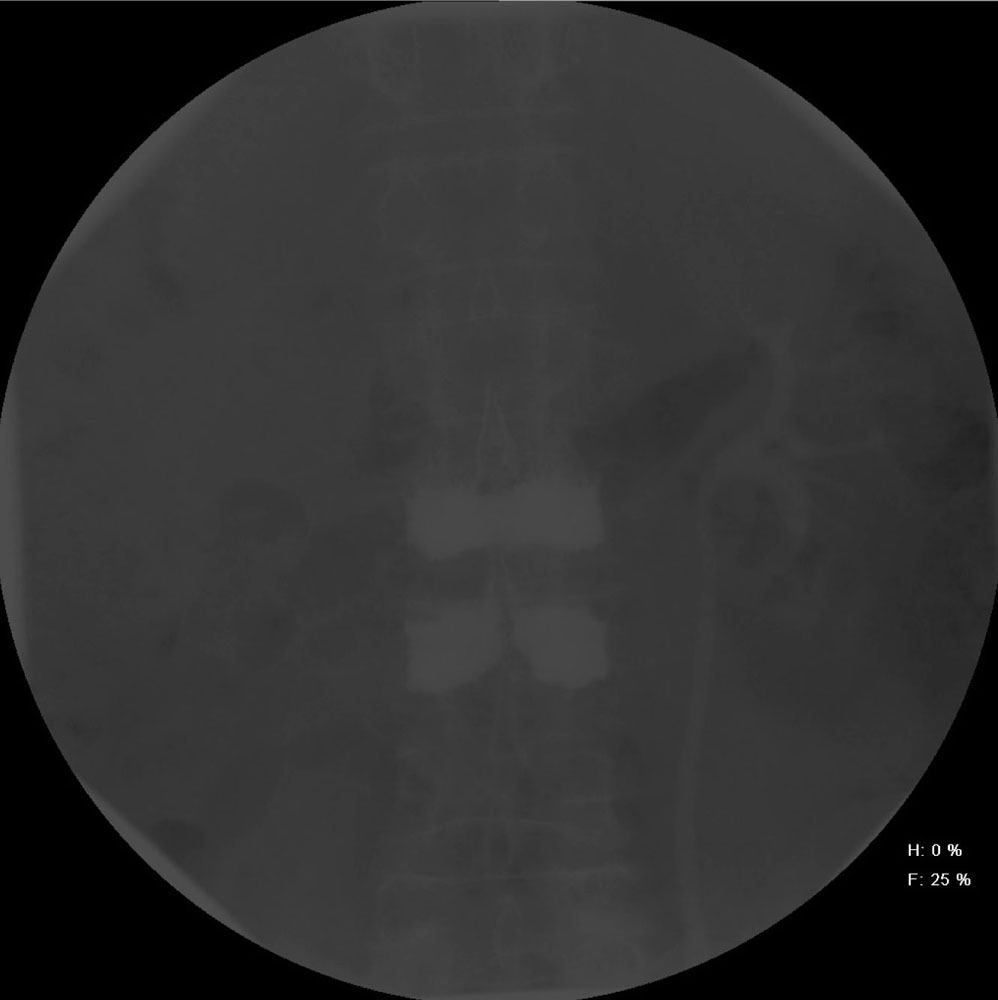
Figure 2. Pretreatment voiding cystourethrogram demonstrating left vesicoureteral reflux into the renal pelvis.
The initial presentation and natural history of VUR in adults is different from those in pediatric populations. Adults are often symptomatic, with recurrent urinary tract infection and pyelonephritis resulting in impaired renal function and hypertension.
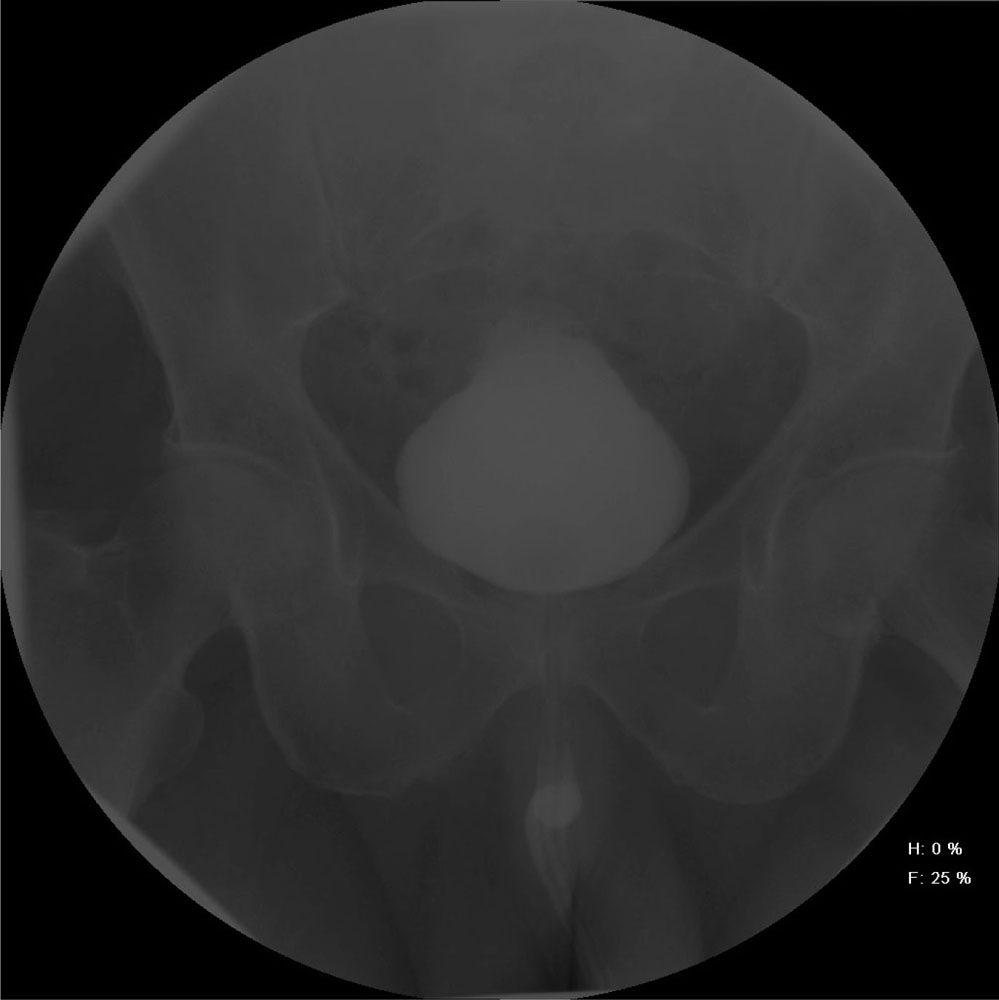
Figure 3. Posttreatment voiding cystourethrogram demonstrating resolved left vesicoureteral reflux.
Main Points
• Advantages relating to endoscopic treatment for vesicoureteral reflux (VUR) in children should be considered when establishing VUR treatment protocols for adults.
• Proven therapeutic benefits in the pediatric population, including shorter hospital stay, minimal postoperative complications, decreased use of long-term antibiotic prophylaxis, and high success rate, are applicable to the adult population.
• Although study experience for adult populations is limited, existing data have proven endoscopic correction with dextranomer/hyaluronic acid to be a safe, minimally invasive, and effective treatment option for VUR.
Main Points
• Advantages relating to endoscopic treatment for vesicoureteral reflux (VUR) in children should be considered when establishing VUR treatment protocols for adults.
• Proven therapeutic benefits in the pediatric population, including shorter hospital stay, minimal postoperative complications, decreased use of long-term antibiotic prophylaxis, and high success rate, are applicable to the adult population.
• Although study experience for adult populations is limited, existing data have proven endoscopic correction with dextranomer/hyaluronic acid to be a safe, minimally invasive, and effective treatment option for VUR.
Vesicoureteral reflux (VUR), though more commonly diagnosed in children, may present in adults and require management. Currently, there is limited evidence to support endoscopic management of VUR with dextranomer/hyaluronic acid (Dx/HA) in adults. We report a case of an elderly man presenting with recurrent episodes of pyelonephritis caused by high-grade VUR. This patient underwent successful management of VUR by endoscopic, subuteric injection of Dx/HA.
Case Report
A 74-year-old man presented for evaluation after discovery of a 3-cm left bladder wall tumor. He underwent transurethral resection of bladder tumor (TURBT). During 3-month follow-up cystoscopy, a recurrent 1.5-cm tumor was identified on the left posterior bladder wall. He returned to the operating room for repeat TURBT, circumcision, and administration of intravesical mitomycin C. He completed a 6-week induction course of bacillus Calmette-Guérin. Pathology from both tumor resections returned low-grade, Ta urothelial cancer of the bladder. The patient has remained free from bladder cancer for 7 years.
The patient developed balanitis xerotica obliterans 4 years after circumcision, requiring self-dilation with a catheter. He subsequently developed three consecutive episodes of left-sided pyelonephritis. Computed tomography scan and ultrasound revealed no urolithiasis or hydronephrosis. Further investigation with voiding cystourethrogram (VCUG) revealed grade 3, left-sided VUR (Figures 1 and 2). Cystoscopy revealed no recurrent bladder tumors. Treatment options were discussed with the patient and, due to existing comorbidities, he elected treatment with endoscopic Dx/HA injection.
The patient was taken to the operating room, and rigid cystoscopy was performed. A total of 1 mL Dx/HA was injected in a subuteric, 6 o’clock position of the left ureteral orifice. Adequate mounding of the subuteric injection was confirmed.
Postoperative VCUG demonstrated complete resolution of left-sided VUR (Figure 3). This patient has remained symptom free for 8 months after injection, with no episodes of pyelonephritis. The patient continues with annual cystoscopic bladder cancer surveillance.
Discussion
VUR, a common problem in children, is occasionally detected and requires surgical correction in adults.1 The initial presentation and natural history of VUR in adults is different from those in pediatric populations.2 Adults are often symptomatic, with recurrent urinary tract infection (UTI)3 and pyelonephritis resulting in impaired renal function and hypertension. The prevalence of VUR in adult patients with recurrent pyelonephritis is estimated to be between 3% and 9%.2 Furthermore, the spontaneous resolution of VUR observed in children is unusual in adults. Therefore, observation for possible resolution of symptomatic VUR in adults is not a valid treatment option, necessitating the correction of VUR in adults to prevent future morbidity.3
An American Urological Association update from 19984 for the treatment of VUR in adolescents and adults recommends the following: (1) no medical management is needed in VUR grade 1-2 and no history of UTI; (2) medical management with lifelong antibacterial prophylaxis should be considered in the cases of low-grade VUR, shortened life expectancy, and poor surgical risk; (3) surgery is indicated in VUR grade 3 or higher, history of recurrent pyelonephritis, and evidence of nephron loss. Ureteroneocystostomy is the standard procedure to treat high-grade VUR, but carries risks associated with extensive abdominal surgery. Moreover, the procedure and recovery after ureteral reimplantation is more difficult for adult patients because pelvic vascularization has increased and the trigone assumes a deeper retropubic location, making dissection, access to the ureteral orifices, and mobilization of the ureters more challenging.3 Due to the significant complications associated with surgical correction and continuous antibiotic prophylaxis, numerous attempts have been made to develop conservative therapies that might provide successful treatment of VUR. Although the therapeutic management of VUR in children has undergone significant changes, moving from surgical to conservative approach, the optimal therapeutic approach in adults is not well defined in the literature.2
Dx/HA is a sterile, highly viscous gel of dextranomer microspheres (50 mg/mL) in a carrier gel of nonanimal stabilized hyaluronic acid (15 mg/mL), constituting a biocompatible and biodegradable implant. The dextranomer microspheres range in size between 80 to 250 μ. Stabilized hyaluronic acid acts mainly as a carrier, leaving the dextranomer microspheres at the implant site.5 Dx/HA is biodegradable, has no immunogenic properties, and has no potential to cause malignant transformation.6 Since US Food and Drug Administration approval of Dx/HA copolymer as a tissue-augmenting substance for endoscopic correction of VUR, there have been numerous studies confirming the effectiveness of endoscopic treatment of VUR in the pediatric population.1 In contrast, there are very limited study data on the use of Dx/HA for endoscopic treatment of VUR in the adult population.
Five studies have evaluated adult patient populations treated with Dx/HA. The adult patients included in each study population presented with recurrent pyelonephritis, including a large percentage with impaired renal function due to prior infection. After inclusion into the study population, patients were identified to have VUR demonstrated by VCUG. Okeke and colleagues7 analyzed 12 ureteral units (9 patients; age range, 18-41 y), all with grade 2-3 VUR. One endoscopic injection corrected VUR in 8 of 9 patients, as measured by postoperative VCUG at 3 months; in patients with persistent VUR, it was corrected by a second injection. Arce and associates8 analyzed 28 ureteral units (21 patients; age range, 16-48 y), including 18 with high-grade VUR (grades 3-5), injected with Dx/HA vs polydimethylsiloxane. A single endoscopic injection corrected the VUR in 69% of affected ureteral units. The success rate per VUR grade 3, 4, and 5 was 62.5%, 100%, and 0%, respectively. A second endoscopic intervention was needed in seven ureteral units (6 patients) that had persistent VUR on follow-up cystography. The second endoscopic injection corrected VUR in 81% of affected ureteral units. Natsheh and colleagues1 analyzed 81 ureteral units (49 patients; age range, 18-64 y), including 11 patients treated with Dx/HA. The first endoscopic injection corrected VUR in 77.8% of affected ureteral units; 10.6% were corrected after a second endoscopic injection, and 4.8% were corrected after a third endoscopic injection. Murphy and coworkers9 analyzed 24 ureteral units (19 patients; age range, 18-33 y), including 9 units with high-grade VUR (grades 3 and 4). The first endoscopic injection corrected VUR in 79% of affected ureteral units, and 92% were corrected after a second endoscopic injection. Moore and Bolduc3 analyzed 23 ureteral units (14 patients; age range, 12-65 y), including 4 units with high-grade VUR (grades 3 and 4). The first endoscopic injection corrected VUR in 86% of affected ureteral units. Subsequently, three failures were documented after the first injection, but each was resolved after a second injection.
The most important factor for the adult population undergoing surgical correction of VUR is whether endoscopic treatment of VUR with Dx/HA injections can prevent further renal damage and UTI development.10 A retrospective evaluation of pediatric data collected by Natsheh and collegues1 and Chertin and associates10 demonstrated that successful endoscopic correction of VUR is accompanied by a low incidence of new renal scarring and febrile UTI, suggesting kidney parenchymal protection. A further decline in renal function postoperatively was only observed in renal units with severe preoperative parenchymal scarring.10 Additionally, only 2.2% of patients were found to develop febrile UTI postoperatively.10 These data are similar to other studies completed in the pediatric setting, including Wadie and colleagues11 and Lackgren and colleagues12 that demonstrated that endoscopic correction of VUR with Dx/HA reduces postoperative incidence of recurrent UTI and pyelonephritis to rates of 8% to 13%. Endoscopic correction with Dx/HA has been shown to reduce recurrent infection and progressive kidney damage in the pediatric population. Therefore, it can be suggested that endoscopic correction of VUR with Dx/HA should be offered as a primary treatment option for the prevention of recurrent infection and kidney damage in adult patients.
Few studies have evaluated the long-term durability of Dx/HA. Many pediatric studies are plagued by short follow-up of 3 to 6 months. Currently, only pediatric and adult patients with symptomatic febrile UTI undergo VCUG to evaluate recurrence of VUR. Natsheh and colleagues1 reported that the main goal of surgical correction in the pediatric population is to prevent development of febrile UTI, and routine VCUG was not offered to all patients who developed recurrent afebrile UTI, unless deterioration of the renal parenchyma was demonstrated through ultrasound examination. As Dx/HA is now the standard of care for VUR in pediatric populations, more data concerning durability will become available as evaluation continues throughout childhood. Likewise, the long-term durability of VUR correction utilizing Dx/HA in adult patients needs to be further investigated.
The use of subuteric, endoscopic injection of Dx/HA for management of VUR in children is well supported in the literature. There are limited data supporting the endoscopic treatment of VUR with Dx/HA in adult populations. The same advantages relating to endoscopic treatment for VUR in children should be considered when establishing VUR treatment protocols for adults. The same arguments that apply in the pediatric population of high success rates, short hospital stay, minimal postoperative complications, and relative low cost compared with long-term antibiotic prophylaxis, should also apply to adults.2 Though study experience for adult populations is limited, existing data have proven endoscopic correction with Dx/HA to be a safe, minimally invasive, and effective treatment option for VUR. To our knowledge, this 81-year-old man may represent the oldest patient in the literature with VUR, who was successfully treated by endoscopic injection of Dx/HA. ![]()
References
- Natsheh A, Shenfeld O, Farkas A, Chertin B. Endoscopic treatment of vesicoureteral reflux in an adult population: can we teach our adult urology colleagues? J Pediatr Urol. 2010;6:600-604.
- Zilberman D, Mor Y. Has the data efflux regarding the promising outcome following injection of deflux changed the management of adult vesicoureteral reflux? Adv Urol. 2008;361324.
- Moore K, Bolduc S. Treatment of vesicoureteral reflux in adults by endoscopic injection. Urology. 2011;77:1284-1287.
- Erhard M, Walker R, Lim D. Management of vesicoureteral reflux in adolescents and adults. AUA Update Series Lesson 5. 1998;17:34-39.
- Deflux [package insert]. Raleigh, NC: Salix Pharmaceuticals, Inc; 2013.
- Stenberg A, Larsson E, Lingholm A, et al. Injectable dextranomer-based implant: histopathology, volume changes and DNA-analysis. Scand J Urol Nephrol. 1999;33:355-361.
- Okeke Z, Fromer D, Katz MH, et al. Endoscopic management of vesicoureteral reflux in women presenting with pyelonephritis. J Urol. 2006;176:2219-2221.
- Arce J, Angerri O, Caffaratti J, et al. Efficiency of endoscopic treatment for vesico-ureteric reflux in adults. BJU Int. 2008;103:71-74.
- Murphy AM, Ritch CR, Reiley EA, Hensle TW. Endoscopic management of vesicoureteral reflux in adult women. BJU Int. 2010;108:252-254.
- Chertin B, Natsheh A, Fridmans A, et al. Renal scarring and UTI after successful endoscopic correction of vesicoureteral reflux. J Urol. 2009;182(4 suppl):1703-1706.
- Wadie GM, Tirabassi MV, Courtney RA, Moriaty KP. The deflux procedure reduces the incidence of urinary tract infections in patients with vesicoureteral reflux. J Laparoendosc Adv Surg Tech A. 2007;17:353-359.
- Läckgren G, Wåhlin N, Sköldenberg E, Stenberg A. Long-term follow-up of children treated with dextranomer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol. 2001;166:1887-1892.