Acromegaly Presenting as Erectile Dysfunction: Case Reports and Review of the Literature
Jerry A. Raju, BMBCh, MA (Oxon), MRCS,1 Kate E. Shipman, BMBCh, MA (Oxon), MRCP, FRCPath,2 John A. Inglis, MBChB, MD, FRCS,1Rousseau Gama, MBChB, MD, FRCP, FRCPath2,3
1New Cross Hospital, Urology Department, Wolverhampton, United Kingdom; 2New Cross Hospital, Clinical Chemistry Department, Wolverhampton, United Kingdom; 3Research Institute in Healthcare Science, University of Wolverhampton, Wolverhampton, United Kingdom
Erectile dysfunction (ED) is a common yet complex condition. The authors report two cases of acromegaly presenting with ED and hypogonadotropic hypogonadism. Surgical cure of the acromegaly was associated with either an improvement or resolution of hypogonadotropic hypogonadism-associated ED. Active acromegaly should be considered in the differential diagnosis of ED presenting with supporting clinical features, particularly hypogonadotropic hypogonadism.
[Rev Urol. 2015;17(4):246-249 doi: 10.3909/riu0676]
© 2016 MedReviews®, LLC
Acromegaly Presenting as Erectile Dysfunction: Case Reports and Review of the Literature
Jerry A. Raju, BMBCh, MA (Oxon), MRCS,1 Kate E. Shipman, BMBCh, MA (Oxon), MRCP, FRCPath,2 John A. Inglis, MBChB, MD, FRCS,1Rousseau Gama, MBChB, MD, FRCP, FRCPath2,3
1New Cross Hospital, Urology Department, Wolverhampton, United Kingdom; 2New Cross Hospital, Clinical Chemistry Department, Wolverhampton, United Kingdom; 3Research Institute in Healthcare Science, University of Wolverhampton, Wolverhampton, United Kingdom
Erectile dysfunction (ED) is a common yet complex condition. The authors report two cases of acromegaly presenting with ED and hypogonadotropic hypogonadism. Surgical cure of the acromegaly was associated with either an improvement or resolution of hypogonadotropic hypogonadism-associated ED. Active acromegaly should be considered in the differential diagnosis of ED presenting with supporting clinical features, particularly hypogonadotropic hypogonadism.
[Rev Urol. 2015;17(4):246-249 doi: 10.3909/riu0676]
© 2016 MedReviews®, LLC
Acromegaly Presenting as Erectile Dysfunction: Case Reports and Review of the Literature
Jerry A. Raju, BMBCh, MA (Oxon), MRCS,1 Kate E. Shipman, BMBCh, MA (Oxon), MRCP, FRCPath,2 John A. Inglis, MBChB, MD, FRCS,1Rousseau Gama, MBChB, MD, FRCP, FRCPath2,3
1New Cross Hospital, Urology Department, Wolverhampton, United Kingdom; 2New Cross Hospital, Clinical Chemistry Department, Wolverhampton, United Kingdom; 3Research Institute in Healthcare Science, University of Wolverhampton, Wolverhampton, United Kingdom
Erectile dysfunction (ED) is a common yet complex condition. The authors report two cases of acromegaly presenting with ED and hypogonadotropic hypogonadism. Surgical cure of the acromegaly was associated with either an improvement or resolution of hypogonadotropic hypogonadism-associated ED. Active acromegaly should be considered in the differential diagnosis of ED presenting with supporting clinical features, particularly hypogonadotropic hypogonadism.
[Rev Urol. 2015;17(4):246-249 doi: 10.3909/riu0676]
© 2016 MedReviews®, LLC
Key words
Erectile dysfunction • Endocrine dysfunction • Endocrinology • Acromegaly • Growth hormone
Key words
Erectile dysfunction • Endocrine dysfunction • Endocrinology • Acromegaly • Growth hormone
Pituitary function tests were diagnostic of active acromegaly with hypogonadotropic hypogonadism and hyperprolactinemia.
GH has been implicated in penile erectile function directly, possibly through the nitric oxide cyclic guanosine monophosphate pathway.
Our first case was unusual because the low GH level and apparent suppression of GH during OGGT is discordant with the diagnosis of acromegaly.
Main Points
• Erectile dysfunction (ED) can be a symptom of numerous underlying conditions, and guidelines on management of ED outline assessment for reversible hormonal causes such as hypogonadism, thyroid dysfunction, and hyperprolactinemia. Although hypogonadism and hyperprolactinemia have been shown to be associated with acromegaly, the link between acromegaly and ED has not been widely reported.
• Acromegaly is a rare condition characterized by growth hormone (GH) hypersecretion. However, it is not widely appreciated that ED and reduced libido are recognized features of acromegaly; up to 35% of patients report ED, although the mechanisms of action are unclear.
• GH has been implicated in penile erectile function directly, possibly through the nitric oxide cyclic guanosine monophosphate pathway.
• Biochemical diagnosis of acromegaly is made by measuring insulin-like growth factor-1 levels; if elevated, GH levels should be measured via a standard 75-g oral glucose tolerance test.
Main Points
• Erectile dysfunction (ED) can be a symptom of numerous underlying conditions, and guidelines on management of ED outline assessment for reversible hormonal causes such as hypogonadism, thyroid dysfunction, and hyperprolactinemia. Although hypogonadism and hyperprolactinemia have been shown to be associated with acromegaly, the link between acromegaly and ED has not been widely reported.
• Acromegaly is a rare condition characterized by growth hormone (GH) hypersecretion. However, it is not widely appreciated that ED and reduced libido are recognized features of acromegaly; up to 35% of patients report ED, although the mechanisms of action are unclear.
• GH has been implicated in penile erectile function directly, possibly through the nitric oxide cyclic guanosine monophosphate pathway.
• Biochemical diagnosis of acromegaly is made by measuring insulin-like growth factor-1 levels; if elevated, GH levels should be measured via a standard 75-g oral glucose tolerance test.
Erectile dysfunction (ED), defined as an inability to obtain or maintain penile erection sufficient for sexual activity, is a common complaint with often complex etiology. Prevalence increases with age, ranging from 1% to 10% of men under age 40, 20% to 40% of men age 60 to 69 years, and 50% to 100% of men in their 70s and 80s.1 ED can be a symptom of numerous underlying conditions, and guidelines on management of ED outline assessment for reversible hormonal causes such as hypogonadism, thyroid dysfunction, and hyperprolactinemia.2,3 Although hypogonadism and hyperprolactinemia have been shown to be associated with acromegaly,4 the link between acromegaly and ED has not been widely reported.5,6 We describe two cases of acromegaly with ED as the presenting feature and review the outpatient diagnosis of acromegaly.
Case Reports
Case 1
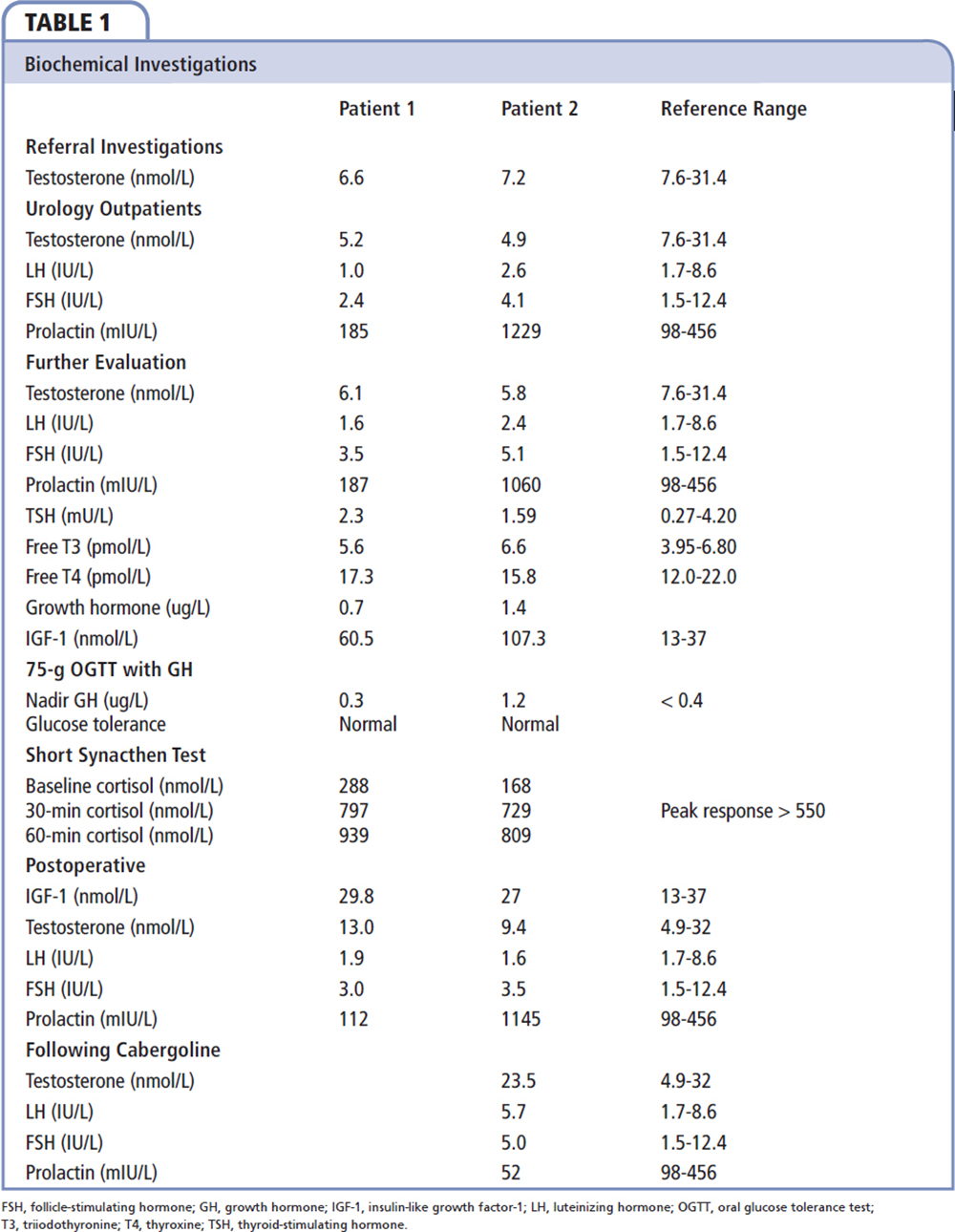
A 43-year-old man with treated hypertension and obstructive sleep apnea was referred with a history of ED associated with reduced libido and low early-morning testosterone levels (Table 1). Apart from obesity (body mass index [BMI], 39.4 kg/m2), results of his physical examination were normal. Initial investigations indicating hypogonadotropic hypogonadism resulted in referral for further investigation. A persistently elevated insulin-like growth factor (IGF)-1 level, albeit with normal growth hormone (GH) study results, led to a diagnosis of active acromegaly with hypogonadotropic hypogonadism (Table 1). Magnetic resonance imaging (MRI) showed a pituitary microadenoma. Hypophysectomy cured the acromegaly and associated hypogonadotropic hypogonadism. He rated his erectile function on presentation at 15 of 25 on the International Index of Erectile Function (IIEF)-5 questionnaire, which improved to 25 of 25 following cure of his acromegaly. After surgery, he lost 10 kg in weight and showed improvements in both obstructive sleep apnea and hypertension.
Case 2
A 38-year-old man with β-thalassemia trait was referred with a 4-month history of worsening erectile function, loss of libido, fatigue, and low early-morning testosterone levels (Table 1). Initial investigations indicating hypogonadotropic hypogonadism and mild hyperprolactinemia resulted in referral for further evaluation. On examination he was overweight (BMI, 29.8 kg/m2) and clinically acromegalic. Pituitary function tests were diagnostic of active acromegaly with hypogonadotropic hypogonadism and hyperprolactinemia (Table 1). A pituitary MRI revealed a left-sided pituitary macroadenoma without stalk compression. Transsphenoidal hypophysectomy cured the acromegaly and normalized serum testosterone concentrations, but the mild hyperprolactinemia persisted. Although the patient noted significant improvement in facial features after surgery, his erectile dysfunction (although improved) was still problematic. He was subsequently prescribed cabergoline, a dopamine receptor D2 agonist, which suppressed his prolactin production, leading to an increase in serum testosterone concentration and a notable improvement in erectile function. On presentation, the patient reported severe ED with an IIEF-5 score of 7 of 25, which did not improve significantly following surgery; however, his IIEF-5 score improved to 14 of 25 after commencement of cabergoline.
Discussion
Acromegaly is a rare condition characterized by GH hypersecretion; it has an insidious onset and a prevalence of 40 to 70 cases per million.7 Over 90% of cases are due to a benign GH-secreting pituitary adenoma. Approximately 25% of these adenomas cosecrete prolactin.8Excess GH secretion causes soft tissue and bony overgrowth, resulting in a wide spectrum of clinical features, including enlargement of the hands and feet, as well as the facial bones and visceral organs. Local pituitary tumor mass effect may cause headache and visual field defects. Cardiovascular complications, including hypertension, cardiomyopathy, and cardiac failure, may ensue. A range of endocrine and metabolic disturbances are also described.8
However, it is not widely appreciated that ED and reduced libido are recognized features of acromegaly; up to 35% of patients report ED,5,6 but the mechanisms of action are unclear. Hypotheses include mass effect with compression of the pituitary gland and stalk, causing hypogonadism and hyperprolactinemia.5 GH has been implicated in penile erectile function directly, possibly through the nitric oxide cyclic guanosine monophosphate pathway.5,6 Similarities in GH and prolactin receptors have also raised the possibility of excess GH mimicking effects of prolactin, which, in high levels, has been linked to sexual dysfunction.6
Biochemical diagnosis of acromegaly is made by measuring IGF-1 levels and, if elevated, measuring GH levels during a standard 75-g oral glucose tolerance test (OGTT). Inadequate GH suppression (,0.4 ug/L) during an OGTT is diagnostic of acromegaly. Pituitary MRI with gadolinium contrast enhancement can then identify and characterize the likely adenoma. Over 75% of pituitary adenomas are macroadenomas (.10 mm in diameter).8 In very rare cases of acromegaly, abdominal and chest imaging may be indicated to detect extrapituitary tumors secreting GH-releasing factor.8 Our first case was unusual because the low GH level and apparent suppression of GH during OGTT is discordant with the diagnosis of acromegaly. This illustrates the diagnostic importance of measuring serum IGF-1, which, if significantly elevated, is diagnostic of acromegaly as false-positive results are extremely rare.
Early morning testosterone measurement for all patients is recommended by ED guidelines and the cause of hypogonadism, if identified, sought.2,3,9 Reversible hormonal causes of ED include hypogonadism, hyperthyroidism, hypothyroidism, and hyperprolactinemia,2 but acromegaly is not mentioned by any major guideline. If testosterone level is low, repeat testing is recommended with prolactin, follicle-stimulating hormone, and luteinizing hormone9; if results are abnormal, referral to a specialist is recommended. Acromegaly may cause ED by non-androgen mechanisms, particularly if euprolactinemic and eugonadal; therefore, the diagnosis of acromegaly should be considered in rare cases of ED presenting with supporting clinical features.
Our cases demonstrate that patients presenting with ED need to be thoroughly assessed to exclude organic and potentially reversible causes of their symptoms. On presentation, our patients were found to have hypogonadotropic hypogonadism with and without hyperprolactinemia. Referral to an endocrine specialist facilitated the rare diagnosis of acromegaly. In view of the significant systemic and local consequences of the disease, this diagnosis was crucial in implementing appropriate long-term management for these patients. ![]()
References
- Lewis RW, Fugl-Meyer KS, Corona G, et al. Definitions/epidemiology/risk factors for sexual dysfunction. J Sex Med. 2010;7(4 Pt 2):1598-1607.
- Hackett G, Kell P, Ralph D, et al; British Society for Sexual Medicine. British Society for Sexual Medicine guidelines on the management of erectile dysfunction. J Sex Med. 2008;5:1841-1865.
- Hatzimouratidis K, Amar E, Eardley I, et al; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010;57:804-814.
- Katznelson L, Kleinberg D, Vance ML, et al. Hypogonadism in patients with acromegaly: data from the multi-centre acromegaly registry pilot study. Clin Endocrinol. 2001;54:183-188.
- Galdiero M, Pivonello R, Grasso LF, et al. Growth hormone, prolactin, and sexuality. J Endocrinol Invest. 2012;35:782-794.
- Maggi M, Buvat J, Corona G, et al. Hormonal causes of male sexual dysfunctions and their management (hyperprolactinemia, thyroid disorders, GH disorders, and DHEA). J Sex Med. 2013;10:661-677.
- Peacey SR, Shalet SM. Insulin-like growth factor 1 measurement in diagnosis and management of acromegaly. Ann Clin Biochem. 2001;38(Pt 4):297-303.
- Melmed S. Medical progress: acromegaly. N Engl J Med. 2006;355:2558-2573.
- Clinical knowledge summaries: erectile dysfunction. National Institute for Health and Care Excellence. http://cks.nice.org.uk/erectile-dysfunction.