Testicular Sclerosing Sertoli Cell Tumor: A Case Report and Review of the Literature
Sarah Coleman, MD,1 Yagil Barazani, MD,1 Andres A. Roma, MD,2 Edmund Sabanegh, Jr, MD1
1Glickman Urological and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH; 2Pathology and Laboratory Medicine Institute, Department of Anatomic Pathology, Cleveland Clinic Foundation, Cleveland, OH
Sertoli cell tumors are very rare testicular tumors, representing 0.4% to 1.5% of all testicular malignancies. They are subclassified as classic, large-cell calcifying, and sclerosing Sertoli cell tumors (SSCT) based on distinct clinical features. Only 42 cases of SSCTs have been reported in the literature. We present a case of a 23-year-old man diagnosed with SSCT.
[Rev Urol. 2014;16(4):191-193 doi: W.3909/riu0620]
© 2014 MedReviews®, LLC
Testicular Sclerosing Sertoli Cell Tumor: A Case Report and Review of the Literature
Sarah Coleman, MD,1 Yagil Barazani, MD,1 Andres A. Roma, MD,2 Edmund Sabanegh, Jr, MD1
1Glickman Urological and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH; 2Pathology and Laboratory Medicine Institute, Department of Anatomic Pathology, Cleveland Clinic Foundation, Cleveland, OH
Sertoli cell tumors are very rare testicular tumors, representing 0.4% to 1.5% of all testicular malignancies. They are subclassified as classic, large-cell calcifying, and sclerosing Sertoli cell tumors (SSCT) based on distinct clinical features. Only 42 cases of SSCTs have been reported in the literature. We present a case of a 23-year-old man diagnosed with SSCT.
[Rev Urol. 2014;16(4):191-193 doi: W.3909/riu0620]
© 2014 MedReviews®, LLC
Testicular Sclerosing Sertoli Cell Tumor: A Case Report and Review of the Literature
Sarah Coleman, MD,1 Yagil Barazani, MD,1 Andres A. Roma, MD,2 Edmund Sabanegh, Jr, MD1
1Glickman Urological and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH; 2Pathology and Laboratory Medicine Institute, Department of Anatomic Pathology, Cleveland Clinic Foundation, Cleveland, OH
Sertoli cell tumors are very rare testicular tumors, representing 0.4% to 1.5% of all testicular malignancies. They are subclassified as classic, large-cell calcifying, and sclerosing Sertoli cell tumors (SSCT) based on distinct clinical features. Only 42 cases of SSCTs have been reported in the literature. We present a case of a 23-year-old man diagnosed with SSCT.
[Rev Urol. 2014;16(4):191-193 doi: W.3909/riu0620]
© 2014 MedReviews®, LLC
Key words
Testicular neoplasm • Sertoli cell tumor • Sclerosing Sertoli cell tumor
Key words
Testicular neoplasm • Sertoli cell tumor • Sclerosing Sertoli cell tumor
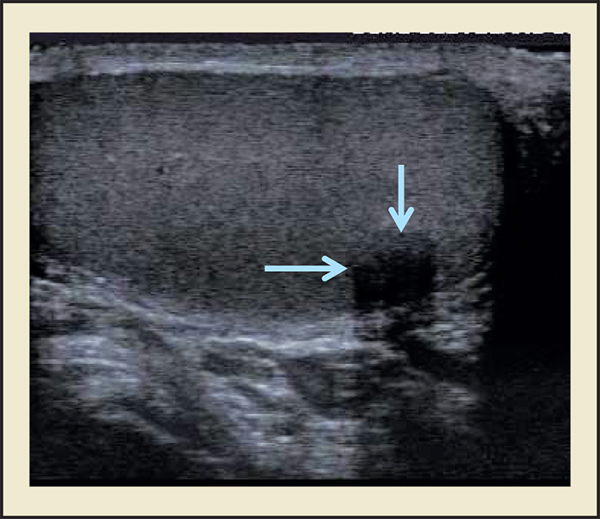
Figure 1. Testicular ultrasound demonstrating an 8 mm × 6 mm × 6 mm hypoechoic, solid mass in the posterior right testicle (blue arrows).
Pathologic examination revealed a grossly unifocal, wellcircumscribed, white, firm mass of 0.8 cm.
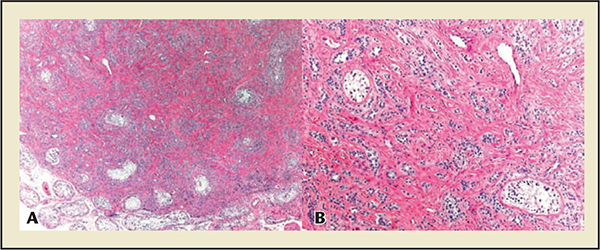
Figure 2. (A) Low-power examination revealing a well-circumscribed tumor composed of solid and hollow tubules and occasional anastomosing cords distributed within the hypocellular, densely collagenous stroma. Hematoxylin and eosin stain, original magnification ×40. (B) High-power examination. Note entrapped seminiferous tubules lacking spermatogenesis. Hematoxylin and eosin stain, original magnification ×100.
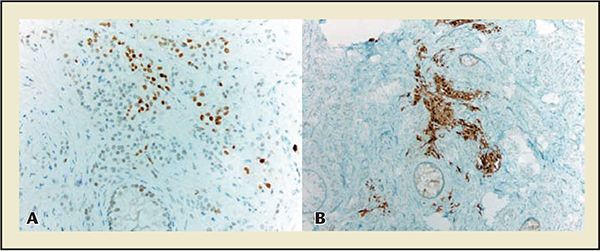
Figure 3. (A) Nuclear expression of steroidogenic factor 1 in the tumor as well as benign Sertoli cells in entrapped seminiferous tubules (original magnification ×200). (B) Focal calretinin expression in the tumor (inhibin had a similar staining pattern; original magnification ×100).
Histopathology demonstrates a uniform pattern of tubules, cords, and aggregates of Sertoli cells separated by extensive sclerotic stroma.
Main Points
• Sertoli cell tumors of the testis are rare, with low malignant potential.
• All reported cases are in postpubertal men without any extratesticular manifestations.
• An intraoperative diagnosis may allow for less aggressive surgical therapy.
Main Points
• Sertoli cell tumors of the testis are rare, with low malignant potential.
• All reported cases are in postpubertal men without any extratesticular manifestations.
• An intraoperative diagnosis may allow for less aggressive surgical therapy.
A 23-year-old man was referred to the Cleveland Clinic Department of Urology (Cleveland, OH) for an incidentally detected right testicular mass. The mass was identified during a work-up for transient left testicular discomfort. His only notable medical history was nephrolithiasis. There was no personal or family history of testicular cancer or cryptorchidism. On physical examination, he was a well-nourished, well-masculinized young man without gynecomastia. Testicular examination revealed normal volume and consistency bilaterally without other relevant findings. Testicular ultrasonography demonstrated an 8 mm × 6 mm × 6 mm hypoechoic, solid mass in the posterior right testicle with peripheral flow on color Doppler (Figure 1).
The remainder of the ultrasound examination yielded normal results. Lactic dehydrogenase, B-human chorionic gonadotropin, and α-fetoprotein levels were all within the normal range. After a thorough review of the options, the patient was then taken to the operating room for inguinal exploration. Intraoperative ultrasound confirmed a superficial 8-mm hypoechoic testis lesion. A white-yellow, well-demarcated nodule was widely excised and a frozen section was sent to pathology for examination. The frozen section examination revealed the lesion to be a neoplasm with differential diagnosis including sclerosing Sertoli cell tumor (SSCT), adenomatoid tumor, and a variant of Leydig cell tumor. Because the final diagnosis could not be determined from frozen section, the decision was made to perform a right radical orchiectomy. Pathologic examination revealed a grossly unifocal, well-circumscribed, white, firm mass of 0.8 cm. Microscopically the lesion was composed of solid and hollow tubules and occasional anastomosing cords distributed within the hypocellular, densely collagenous stroma. Although the lesion was somewhat well circumscribed, entrapped seminiferous tubules with Sertoli-only cells were present within the tumor (Figure 2). Tumor cells had pale or eosinophilic cytoplasm with small and dark nuclei with inconspicuous nucleoli. The tumor was confined to the testis and margins were negative. A diagnosis of SSCT was reached, supported by positive immunostain results for steroido-genic factor 1, focal inhibin, and calretinin expression, and negative stain results for cytokeratin AE1/AE3 and epithelial membrane antigen in the tumor (Figure 3). The postoperative course was unremarkable. Computed tomography scan of the abdomen and pelvis and chest radiograph were negative for metastatic disease.
Discussion
Sertoli cell tumors of the testis are a very rare neoplasm with three identified subtypes: general, large-cell calcifying, and sclerosing Sertoli cell.1 Zuckerberg and colleagues1 first identified the SSCT variant in a case series of 10 patients in 1991. To date, 43 case reports have been published in the literature including the case presented here.1-8 This rare variant of Sertoli cell tumors has been reported exclusively in postpubertal men ranging in age from 18 to 80 years. All cases have been reported as unilateral without evidence of feminization or extra-testicular manifestations. This presentation is in contrast to the large-cell calcifying type of Sertoli cell tumor that leads to increased estrogen production and gyneco-mastia in 11% to 25% of reported cases.9 Metastatic disease has been reported in one patient in a recent series by Kao and colleagues.8 This patient presented with metastatic disease to the bone and died of his disease 27 months after presentation. One patient was found to have pathologic characteristics consistent with malignancy (frequent mitosis, cellular atypia, rete testis, and epididymis infiltration); however, he died from cardiac disease 5 years after presentation and an autopsy was not performed.1
SSCTs are typically small (0.4-1.5 cm, maximum 4 cm),4 whereas the other subtypes can be significantly larger.1,4 Histopathology demonstrates a uniform pattern of tubules, cords, and aggregates of Sertoli cells separated by extensive sclerotic stroma. Extensive sclerosis is present as compared with focal sclerosis observed in general and large-cell calcifying Sertoli cell tumors.1 General Sertoli cell tumors stain positive for cytokeratin, an intermediate filament protein found in epithelial cells and tumors, in contrast to SSCTs, which are negative for cytokeratin expression.
The large-cell calcifying Sertoli cell subtype has been uniquely associated with precocious puberty, pituitary adenoma, adrenocortical hyperplasia, and cardiac myxoma.8 An association between this subtype and tuberous sclerosis and Peutz-Jeghers syndrome has been described. Such extratesticular manifestations have never been described in the sclerosing subtype, further supporting the clinical significance of the specific subtype assigned to Sertoli cell tumors.
In conclusion, our case adds to the reported literature on SSCT, a rare subtype of Sertoli cell tumors with low malignant potential. Practicing urologists should be familiar with the known subtypes of SSCT, as these appear amenable to less aggressive surgical therapies such as local excision if the diagnosis can be confirmed intraoperatively. ![]()
The authors report no real or apparent conflicts of interest.
References
- Zuckerberg LR, Young RH, Scully RE. Sclerosing Ser toli cell tumor of the testis. A report of 10 cases. Am J SurgPathol. 1991;15:829-834.
- Anderson GA. Sclerosing Sertoli cell tumor of the testis: a distinct histological subtype. J Urol. 1995:154:1756-1758.
- Gravas S, Papadimitriou K, Kyriakidis A. Sclerosing sertoli cell tumor of the testis—a case report and review of the literature. Scand J Urol Nephrol. 1999:33:197-199.
- Giglio M, Medica M, De Rose AF, et al. Testicular sertoli cell tumours and relative sub-types. Analysis of clinical and prognostic features. Urol Int. 2003:70:205-210.
- Abbas F, Bashir NW, Hussainy AS. Sclering Sertoli cell tumor of the testis. J Coll Physicians Surg Pak. 2005:15:437-438.
- Esber CM, Shabsigh A, Zynger DL. Sclerosing Sertoli cell tumor without expression of typical sex cord stromal tumor markers: Case report and literature review. Pathol Res Pmct. 2012:208:121-125.
- Brunocilla E, Pultrone CV, Schiavina R, et al. Testicular sclerosing Sertoli cell tumor: an additional case and review of the literature. Anticancer Res. 2012;32: 5127-5130.
- Kao SC, Kum JB, Idrees MT, Ulbright TM. Sclerosing Sertoli cell tumor of the testis: a clinicopathologic study of 20 cases. Am J Surg Path. 2014:38:510-517.
- Proppe KH, Scully RE. Large-cell calcifying Sertoli cell tumor of the testis. Am J Clin Pathol. 1980:74: 607-619.