Pulmonary Valve Papillary Fibroelastoma: A Rare Tumor and Rare Location
Hatim Yagoub, MBBS, MSc,1 Abdullah Sayied Abdullah, MBBS, MRCPI,1 Abdalla Ibrahim, MBBS,1 Brendan Meany, MRCPI,1 Peter Faul, MB,2 Thomas J. Kiernan, MD1
1Cardiology Department, University Hospital Limerick, Ireland; 2Pathology Department, University Hospital Limerick, Ireland
Although rare, papillary fibroelastomas (PFEs) are considered the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography. PFEs of the pulmonary valve are extremely rare. They are usually benign; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed. This article reviews a case of an asymptomatic PFE of the pulmonary valve, incidentally found in a patient who presented with three-vessel coronary artery disease.
[Rev Cardiovasc Med. 2015;16(1):90-93 doi: 10.3909/ricm0757]
© 2015 MedReviews®, LLC
Pulmonary Valve Papillary Fibroelastoma: A Rare Tumor and Rare Location
Hatim Yagoub, MBBS, MSc,1 Abdullah Sayied Abdullah, MBBS, MRCPI,1 Abdalla Ibrahim, MBBS,1 Brendan Meany, MRCPI,1 Peter Faul, MB,2 Thomas J. Kiernan, MD1
1Cardiology Department, University Hospital Limerick, Ireland; 2Pathology Department, University Hospital Limerick, Ireland
Although rare, papillary fibroelastomas (PFEs) are considered the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography. PFEs of the pulmonary valve are extremely rare. They are usually benign; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed. This article reviews a case of an asymptomatic PFE of the pulmonary valve, incidentally found in a patient who presented with three-vessel coronary artery disease.
[Rev Cardiovasc Med. 2015;16(1):90-93 doi: 10.3909/ricm0757]
© 2015 MedReviews®, LLC
Pulmonary Valve Papillary Fibroelastoma: A Rare Tumor and Rare Location
Hatim Yagoub, MBBS, MSc,1 Abdullah Sayied Abdullah, MBBS, MRCPI,1 Abdalla Ibrahim, MBBS,1 Brendan Meany, MRCPI,1 Peter Faul, MB,2 Thomas J. Kiernan, MD1
1Cardiology Department, University Hospital Limerick, Ireland; 2Pathology Department, University Hospital Limerick, Ireland
Although rare, papillary fibroelastomas (PFEs) are considered the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography. PFEs of the pulmonary valve are extremely rare. They are usually benign; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed. This article reviews a case of an asymptomatic PFE of the pulmonary valve, incidentally found in a patient who presented with three-vessel coronary artery disease.
[Rev Cardiovasc Med. 2015;16(1):90-93 doi: 10.3909/ricm0757]
© 2015 MedReviews®, LLC
KEY WORDS
Papillary fibroelastoma • Cardiac neoplasm • Transthoracic echocardiography
KEY WORDS
Papillary fibroelastoma • Cardiac neoplasm • Transthoracic echocardiography
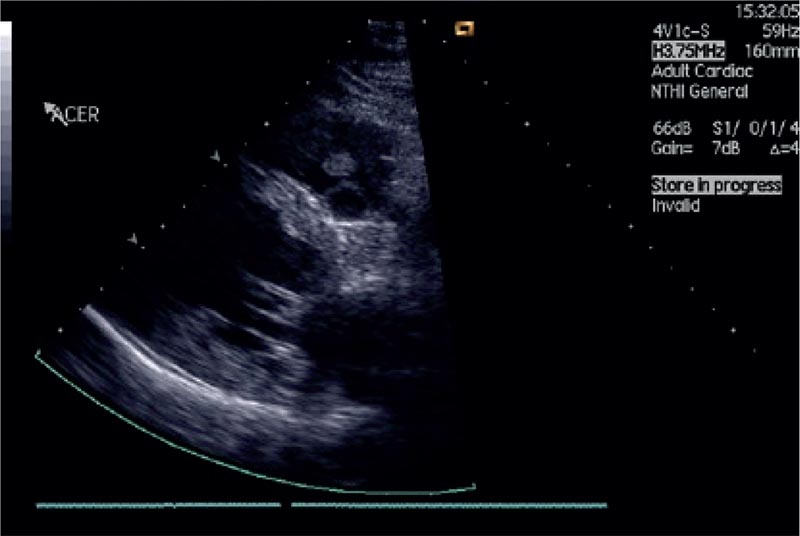
Figure 1. Transthoracic echocardiogram showing an incidental small 1 3 1 cm mobile mass attached to the pulmonary valve with mild pulmonary regurgitation.

Figure 2. Transthoracic echocardiogram revealing an incidental small 1 × 1 cm mobile mass attached to the pulmonary valve with mild pulmonary regurgitation.
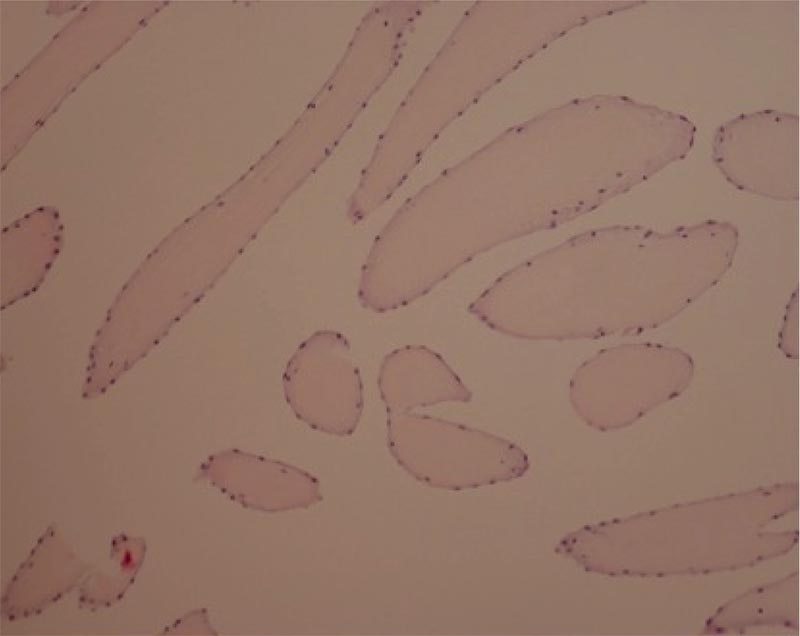
Figure 3. Postoperative histology of the mass showing multiple papillary fronds with dense hyalinized cores and flat endocardial lining, suggestive of papillary fibroblastoma.
As these tumors are generally small in size, transesophageal echocardiography is commonly needed to further characterize the lesions and their attachment…

Figure 4. Percentage of valves affected by papillary fibroelastoma.
Main Points
• Although they are rare, papillary fibroelastomas (PFEs) are considered to be the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography.
• PFEs are usually benign; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed.
• Transesophageal echocardiography is commonly needed to further characterize the lesions and their attachment, and to help differentiate them from other tumors and vegetation. Cardiac magnetic resonance imaging can play a leading role in identifying anatomic and tissue characterization and the functional aspect of the mass.
• Excision is indicated for patients with embolic events and events related to tumor mobility (eg, coronary ostium occlusion). From retrospective data, surgery is recommended for large tumors > 1 cm in size.
Main Points
• Although they are rare, papillary fibroelastomas (PFEs) are considered to be the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography.
• PFEs are usually benign; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed.
• Transesophageal echocardiography is commonly needed to further characterize the lesions and their attachment, and to help differentiate them from other tumors and vegetation. Cardiac magnetic resonance imaging can play a leading role in identifying anatomic and tissue characterization and the functional aspect of the mass.
• Excision is indicated for patients with embolic events and events related to tumor mobility (eg, coronary ostium occlusion). From retrospective data, surgery is recommended for large tumors > 1 cm in size.
Papillary fibroelastomas (PFEs), although rare, are considered to be the third most common cause of primary cardiac neoplasm. They are usually asymptomatic and are found during routine echocardiography. PFEs of the pulmonary valve are very rare. They usually run a very benign course; however, because of their potential to embolize to the pulmonary circulation, it is often recommended that they be removed. We report a case of an asymptomatic PFE of the pulmonary valve, incidentally found in a patient who presented with three-vessel coronary artery disease and was being assessed for coronary artery bypass graft (CABG) surgery.
Case Report
A 75-year-old man with multiple risk factors for coronary artery disease presented with non-ST segment elevation myocardial infarction. His clinical examination was unremarkable. Subsequent coronary angiogram showed severe three-vessel disease. Transthoracic echocardiogram unexpectedly revealed an incidental small 1×1 cm mobile mass attached to the pulmonary valve with mild pulmonary regurgitation (Figures 1 and 2). A provisional diagnosis of primary cardiac tumor was made.
The patient underwent CABG surgery with removal of the mass and repair of the pulmonary valve. Postoperative histology of the mass showed multiple papillary fronds with dense hyalinised cores and flat endocardial lining most suggestive of papillary fibroelastoma (Figure 3). The patient recovered very well, and 1-year follow-up echocardiogram showed no recurrence of the tumor and normal valvular function.
Discussion
Cardiac tumors are relatively rare. Secondary tumors from metastasis to the heart are approximately 30 times more common than primary cardiac neoplasms. Autopsy reports have shown the incidence of primary cardiac tumors to be approximately 0.3%.1 Although all secondary cardiac tumors are malignant by definition, approximately 75% of primary cardiac neoplasms are benign.
PFEs are the third most common primary cardiac tumor after atrial myxomas and lipomas.2 They arise from the valvular endocardium in approximately 80% to 90% of cases, but can also be found on papillary muscles, chordae tendineae, or the endocardium.3,4 When they affect the semilunar valves, they are more likely to be found on the ventricular aspect of the valves, whereas the atrial surface of the valve is the more likely site in cases of PFEs of the atrioventricular valves. The valves affected, in descending order of frequency, are the aortic valve, followed by the mitral, tricuspid, and pulmonary valves (Figure 4). Nonvalvular locations are present in 16% of cases.5 Although these tumors are rarely associated with valvular dysfunction, thromboembolic phenomena (eg, transient ischemic attack or stroke) are the most common presenting feature in cases of left-sided tumors.6,7 Pulmonary embolism or paradoxical embolism to the systemic circulation, secondary to patent foramen ovale, has been observed in right-sided tumors.5
PFEs of the pulmonary valve are extremely rare and data in the literature are relatively scarce. They are usually asymptomatic or may present with pulmonary embolism. They can also be incidental findings on postmortem examination. Macroscopically, the tumor is composed of multiple projections, which makes it friable and more susceptible to embolization or clot formation. It is usually attached to a pedicle or a stalk.4,8 Microscopically, they are avascular papillomas with a single layer of endocardial cells covering the papillary surface. The matrix consists of proteoglycans, elastic fibers, and rarely, spindle cells. The fibrinous matrix is the hallmark of this tumor.9 The origin of PFE is unclear and various possible causes have been mentioned in the literature. They have been considered as hamartomas, organized thrombi, iatrogenic (after radiation or surgery), or inflammatory foci due to unusual endocardial responses to infection or hemodynamic trauma. However, some authors believe that PFEs are true neoplasms.10-13
Diagnosis is suspected on trans-thoracic echocardiography, which is increasingly used, leading to higher rates of detection of asymptomatic tumors.14 As these tumors are generally small in size, transesophageal echocardiography is commonly needed to further characterize the lesions and their attachment, and to help differentiate them from other tumors and vegetation. Cardiac magnetic resonance imaging can play a leading role in identifying anatomic and tissue characterization and the functional aspect of the mass.
Most of the existing data are on the management of left-sided papillary fibroelastoma. Little is available to support any recommendations on the less common right-sided tumors.
Decisions regarding the primary surgical excision of PFE depend on the mobility, size, and potential or strength of association of the tumor with symptoms. The most important independent predictor of adverse outcome with regard to death or embolic events is tumor mobility. Excision is indicated for patients with embolic events and events related to tumor mobility (eg, coronary ostium occlusion). From retrospective data, surgery is recommended for large tumors > 1 cm in size.15 Although anticoagulation can be used to minimize the risk of thromboembolism, this can still occur due to embolization of tumor fragments.5 ![]()
References
- Bisel HF, Wroblewski F, Ladue JS. Incidence and clinical manifestations of cardiac metastases. J Am Med Assoc. 1953;153:712-715.
- Howard RA, Aldea GS, Shapira OM, et al. Papillary fibroelastoma: increasing recognition of a surgical disease. Ann Thorac Surg. 1999;68:1881-1885.
- Klarich KW, Enriquez-Sarano M, Gura GM, et al. Papillary fibroelastoma: echocardiographic characteristics for diagnosis and pathologic correlation. J Am Coll Cardiol. 1997;30:784-790.
- Costa MJ, Makaryus AN, Rosman DR. A rare case of a cardiac papillary fibroelastoma of the pulmonary valve diagnosed by echocardiography. Int J Cardiovasc Imaging. 2006;22:199-203.
- Gowda RM, Khan IA, Nair CK, et al. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am Heart J. 2003;146:404-410.
- Kasarskis EJ, O’Connor W, Earle G. Embolic stroke from cardiac papillary fibroelastomas. Stroke. 1988;19:1171-1173.
- Topol EJ, Biern RO, Reitz BA. Cardiac papillary fibroelastoma and stroke. Echocardiographic diagnosis and guide excision. Am J Med. 1986;80:129-132.
- Daveron E, Jain N, Kelley GP, et al. Papillary fibroelastoma and Lambl’s excrescences: echocardiographic diagnosis and differential diagnosis. Echocardiography. 2005;22:461-463.
- Burke A, Virmani R. Papillary fibroelastoma: tumors of the heart and great vessels. In: Atlas of Tumor Pathology. 3rd Series. Washington, DC: Armed Forced Institute of Pathology; 1996:47-54.
- Grinda JM, Couetil JP, Chauvaud S, et al. Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization. J Thorac Cardiovasc Surg. 1999;117:106-110.
- Law KB, Phillips KRB, Cusimano RJ, Butany J. Multifocal “tapete” papillary fibroelastoma. J Clin Pathol. 2009;62:1066-1070.
- Bicer M, Cikirikcioglu M, Pektok E, et al. Papillary fibroelastoma of the left atrial wall: a case report. J Cardiothorac Surg. 2009;4:28.
- Jha NK, Khouri M, Murphy DM, et al. Papillary fibroelastoma of the aortic valve—a case report and literature review. J Cardiothorac Surg. 2010;5:84.
- Edward FH, Hale D, Cohen A, et al. Primary cardiac valve tumors. Ann Thorac Surg. 1991;52:1127-1131.
- Sydow K, Willems S, Reichenspurner H, Meinertz T. Papillary fibroelastomas of the heart. Thorac Cardiovasc Surg. 2008;56:9-13.