Original Article
Cost Analysis of Premixed Multichamber Bags Versus Compounded Parenteral Nutrition: Breakeven Point
Erkut Bozat, MBA*,†; Gamze Korubuk, Pharm‡; Pelin Onar, Msc§; and Osman Abbasoglu, MD¶
Abstract
Purpose: Industrially premixed multichamber bags or hospital-manufactured compounded products can be used for parenteral nutrition. The aim of this study was to compare the cost of these 2 approaches.
Materials and Methods:Costs of compounded parenteral nutrition bags in an university hospital were calculated. A total of 600 bags that were administered during 34 days between December 10, 2009 and February 17, 2010 were included in the analysis. For quality control, specific gravity evaluation of the filled bags was performed.
Results: It was calculated that the variable cost of a hospital compounded bag was $26.15. If we take the annual fixed costs into consideration, the production cost reaches $36.09 for each unit. It was estimated that the cost for the corresponding multichamber bag was $37.79. Taking the fixed and the variable costs into account, the breakeven point of the hospital compounded and the premixed multichamber bags was seen at 5,404 units per year. In specific gravity evaluation, it was observed that the mean and interval values were inside the upper and lower control margins.
Conclusion: In this analysis, usage of hospital-compounded parenteral nutrition bags showed a cost advantage in hospitals that treat more than 15 patients per day. In small volume hospitals, premixed multichamber bags may be more beneficial.
Key Words—all-in-one admixtures, cost analysis, hospital-compounded bags, parenteral nutrition
Hosp Pharm—2014;49(2):170–176
Hosp Pharm 2014;49(2):170–176
2014 © Thomas Land Publishers, Inc.
doi: 10.1310/hpj4902-170
Parenteral nutrition (PN) is used to provide nutritional support for patients who are unable to consume adequate nutrients via an oral or enteral route. Two types of products for parenteral nutrition are available: industrially premixed multichamber bags and hospital-compounded individualized admixtures. Industrially premixed products, which contain macronutrients and electrolytes in various amounts and volumes, are available commercially. Some hospital pharmacies that have appropriate facilities can locally produce parenteral nutrition solutions that are tailored to the patients’ specific requirements. Considering the health care policy of the local authority, hospitals decide which approach meets their requirements in terms of clinical effectiveness and economical efficiency. Few studies in the literature compare the costs of different PN application systems, and most studies favor the premixed multichamber bags.1-3
The aim of this study was to provide a cost comparison of the administration of hospital-compounded and premixed multichamber bags in PN. From the operational point of view, the production procedures have also been examined and the statistical quality control process has been analyzed.
Experimental Methods
Study Population
This study was performed in an university hospital with 1,200 patient beds that received quality approval by the Joint Commission International (JCI) in 2007 and that has been producing PN solutions in the in-house pharmacy according to GMP (good manufacturing practice) guidelines for the past 15 years. All-in-one admixtures are prepared in a pharmacy-based central intravenous admixture service area on a daily basis, and physico-chemical and microbial stability of the admixtures are tested routinely. GMP is a quality standard (materials, room conditions, equipment, employees, documentation, distribution, etc) that must be followed for manufacturing all-in-one admixtures.4 The current daily output is approximately 20 PN bags for adult patients and 25 PN bags for newborn and pediatric patients. Only adult patients were included in the study; PN formulas were prescribed to meet the patients’ needs by the nutritional support team. In practice, the requirements for energy, protein, and fluid were 25 to 30 kcal, 1.0 to 1.5 g protein, and 30 mL fluid per kg of body weight per day. Vitamins and trace elements were supplemented in the recommended amounts.
Data were evaluated retrospectively for patients receiving PN between December 10, 2009 and February 17, 2010. During these 70 days, a total of 85 patients received 1,370 compounded PN bags. Of these patients, 39 received peripheral, 35 received central, and 11 received both peripheral and central PN. Among these 1,370 PN bags, randomly selected 300 central and 300 peripheral compounded admixtures that were based on standard formulations were included in the analysis.
Statistical Quality Control (Specific Gravity Measurement)
Various methods exist for measuring quality control, one of which is preparing control charts to represent the sample data, such as the X-bar chart and the R chart. This type of procedure generally has been conducted for standard production processes across different industrial areas. Our objective was to adapt this kind of methodology to the hospital manufacturing process. Therefore, we had to compose a uniform sample group of hospital-compounded bags for which we would be able to develop and interpret control charts. As most of the central admixtures are tailored to patient’s needs, peripheral admixtures were selected to achieve more standard formulations. Consequently, we randomly selected certain peripheral admixtures that were used almost every day (43% of the daily hospital-compounded PN bags). The content of the admixtures has been broken down in terms of macronutrients: 824 mL 8.5% standard amino acid solution, 280 mL 20% olive oil–based fat emulsion, 1,235 mL 20% dextrose solution, and 500 mL 0.9% sodium chloride (NaCl) solution.
Measurements of specific gravity were carried out by means of a highly sensitive balance (Precisa XB620 A; Precisa Gravimetrics AG, Dietikon, Switzerland). First, the weights of empty bags were determined. Then, the average weight of 30 bags, which had been selected randomly, was added to all filled bags as a standard value (62,86 g for 2 L container, and 75,23 g for 3 L container). We applied a different method for weighing the filled bags. Just prior to the filling process, a label was affixed to each bag that had been designated for a particular patient, providing data concerning the nutritional components. Next, the filling procedure was performed by the compounding devices. In this study, a conversion calculation was carried out for each component that was available in liquid form and thus presented a value in milliliters. As each liquid had a different concentration, and consequently a different density value, the content of each bag was converted into milligram values according to the label value (mL). In addition, weights of empty bags and labels, which had been accepted as standard values, were included into the calculation. After completing the weighing process to a high degree of accuracy, we matched each measured value with the expected value to determine the standard deviation. To perform statistical methods, different modules of POM-QM for Windows software (Howard J. Weiss) were applied, such as Quality Control and Breakeven Analysis. On the financial side, the fiscal level of given alternatives was represented.
Cost Calculation
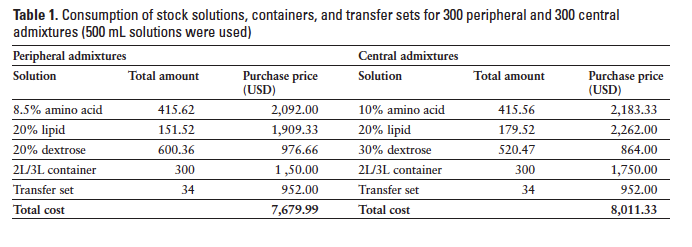
Our methodology for the cost comparison was based on macronutrient contents and fixed costs. As both premixed multichamber and hospital-compounded parenteral solutions do not contain micronutrients, such as vitamins and trace elements, these are added into the admixtures just prior to infusion. These additional costs have been regarded as identical for both groups and have not been included in the analysis. Similarly costs that were identical, such as central venous catheters, dressings, disposal, and transport services, were not included in the calculation. Due to the fact that this hospital does not purchase commercially manufactured multichamber bags, the cost calculation for multichamber bags was based on the prices that manufacturers sell these products to other university hospitals in the same city. The total consumption of stock solutions of amino acid solutions, dextrose, and lipids was determined as listed in Table 1.
In addition to the variable costs, fixed costs were calculated. Fixed costs involve the preparation process for PN solutions when these are compounded from stock solutions in the hospital pharmacy. Fixed costs mainly include labor costs, depreciation expenses of equipment, consumption of disposables, energy consumption, and costs related to cleaning and disinfection. For compounding, Automix 3+3 compounding system (Baxter Healthcare Corp., Deerfield, IL) is used. The laminar flow workstation is placed in a temperature- and humidity-controlled environment. Testing and validating the laminar flow cabinets is done periodically in house. In accordance with the standard operating policies, which apply in most of the European countries, the admixing process must be carried out under the supervision of a pharmacist. Thus, the labor cost of the pharmacist has been included in the calculation, whereas a partial amount of the pharmacist’s salary has been considered as a fixed cost for the premixed multichamber bags. Labor costs also include cleaning, maintenance, and microbial testing. To compare the existing hospital-compounded admixtures with premixed multichamber bags, we considered factors such as total volume, total calories, total nonprotein calories, total protein, and type of lipid emulsion. The costs were based upon the actual volumes used. The price of the premixed multichamber bag that is available in the market that matches best with the compounded formula was used for cost calculation.
Results
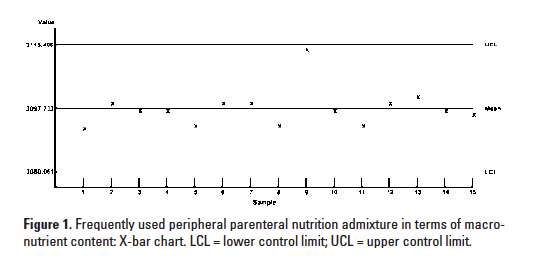
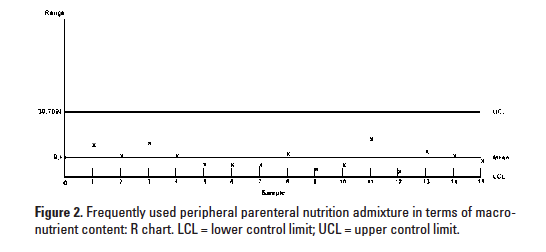
The infrastructure of this university hospital is adequate for compounding parenteral solutions in the hospital pharmacy. The area in which the compounding devices are located is convenient in terms of sterile conditions and operates according to parenteral nutrition GMP guidelines. When the hospital-compounded bags were evaluated in terms of their specific gravity measurement, they met acceptable quality control limits. Mean and interval values of the sample data were within the upper and lower control limits. One can claim that the compounding operates accurately with respect to the process competence.
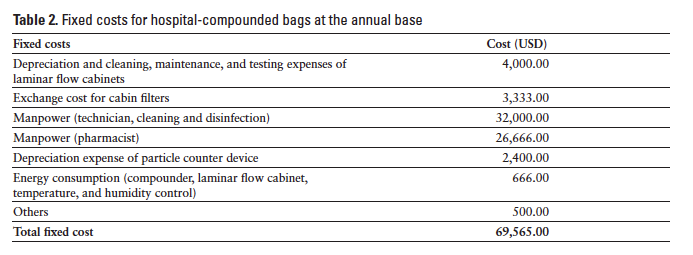
Table 2 shows the fixed costs at the annual base. We prorated the figure obtained for 600 bags to one full year to determine an estimate. If we assume that the annual need for adult PN is 7,000 bags, it is likely that the yearly variable production cost would amount to $183,065. Provided that this institution makes a fixed capital investment of $69,565 at the annual base, the total expenses will be about $252,630 per year. Under these conditions, the final cost per bag will be $36.09; clearly this is an approximate value.
Variable costs, consisting of stock solutions, containers, and transfer sets, constituted the major part (72%) of the total cost. Manpower cost was about 23% of total costs.
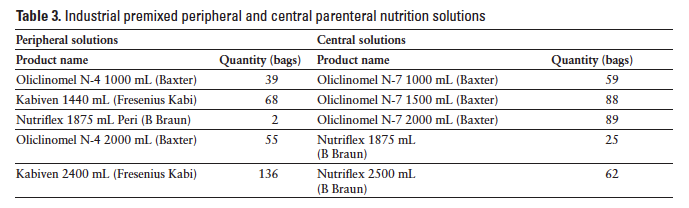
Table 3 demonstrates the distribution of industrial premixed multichamber bags that were considered in the cost analysis. Using our hypothetical approach, the mean PN bag cost for single premixed multichamber bag was found to be $37.79.
Control Diagrams and Process Control for Variables
Control diagrams, such as the X-bar chart and the R chart, are used for monitoring the constant data. A control diagram related to the mean (X-bar) reveals the variability among the sample averages and stresses a deviation that occurs in the process average. An R chart monitors the variability among the samples and points out the variability in the data range. Figures 1 and 2 demonstrate the charts related to the mean and interval of the peripheral PN solutions that have been produced in the hospital pharmacy. As can be observed, X-bar and R values are within the upper and lower limits. It can be claimed that the Automix 3+3 (Baxter Healthcare Corp.) compounding device operates properly and represents reasonable process capability.
Breakeven Point (Cost-Volume Analysis)
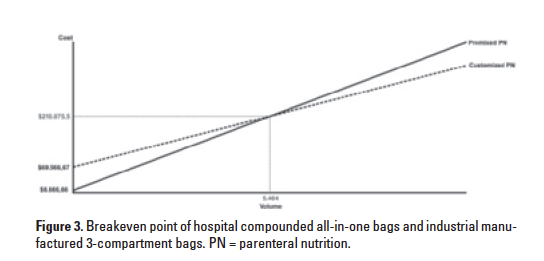
Cost-volume-profit is a form of accounting, and it is a simplified model that is useful for elementary instruction and for short-term decisions. It provides the decision makers with a mathematical model to help them evaluate a current circumstance. A critical part of such analysis is the point at which the values of different options become equal. Figure 3 shows the point at which the costs of hospital-compounded bags and premixed multichamber bags are identical. As stated previously, the annual need for adult PN is approximately 7,000 bags. If we take the fixed and variable costs into account, the breakeven point of hospital-compounded bags and industrial-manufactured products is reached at 5,404 units and $210,876. The point corresponds to nearly 15 admixtures per day. If this hospital uses more than 15 bags per day, hospital compounding seems to have financial advantage.
Discussion
Based on the analysis of the data collected specifically for this purpose, hospital-compounded bags may provide an advantage for those institutions preparing PN for a high volume of patients (more than 15 PN bags per day). In addition to financial issues, patients with specific illnesses, such as renal failure, liver dysfunction, and electrolyte inbalance, and patients with increased metabolic needs may need “tailor-made” regimens. Under these obsevations, it seems reasonable to use componded PN bags for referral hospitals with a high volume of patients.
Very few articles related to this topic have been published to date. Investigations on economical aspects of PN have been conducted in different countries with conflicting results. Financial analysis seems to be country specific and does not necessarily overlap with other markets. Labor costs, for instance, are high and affect the results significantly. Genton et al5 indicated the need for a verification of financial outcomes in countries with low-cost manpower. PN costs differ among countries, and the major variable is staff time. In a multicountry study in Europe, Walter et al6 found that wages accounted for 54% of all costs in PN in children. In this study, average cost per bag for chidren was found to be 80 euros in the United Kingdom and 125 euros in Germany. In the present study, manpower represents 23% of PN hospital costs.
On the other hand, premixed multichamber bags have reasonably low purchasing prices for hospitals in Turkey when compared to many European hospitals. This is mainly due to the discounts; in Turkey, the major reimbursement authority is the Social Security Institution (SSI). SSI has been implementing a practice of major compulsory discount for government hospitals to reduce global medical expenditures. As a result of this policy, pharmaceutical companies may have to give a discount for all pharmaceuticals, which can be as high as 40%. The actual hospital purchasing prices we encountered recently for industrial multichamber bags fall within the range of $14.50 to $35, depending
on the volume and contents of the bags. Depending on the discount rates, hospital costs may change and the cost analysis may not be applicable to other health care institutions. Even if another hospital has been utilizing the same system, the costs will not necessarily be the same.
In our hospital, the pharmacy produces PN bags daily, including weekends and holidays. This is extremely important to decrease waste. In many hospitals, the practice is to admix PN solutions on Friday for the weekend, which results in a 3-day preparation. Considering this fact, patients who do not need PN at any given weekend will not be administered the compounded product, resulting in waste of the admixture and incremental cost. On the other hand, 3-chamber premixed bags are not available and 2-chamber bags are only available in 1 L and 2 L volumes in some countries, including the United States. This would probably cause significant wastage for patients who require
volumes other than those offered by commercial products. Therefore we suggest that hospitals should determine their PN preperation policies according to their practice and regulations. Research on this topic is still needed, as verification of financial analysis becomes more important in today’s health care environment.
In addition to acquisition costs, complications of PN may contribute to final cost analysis. In a multicenter study, Turpin et al7 showed that premixed multichamber bags were associated with lower costs than compounded PN with regard to both PN acqusition and potential avoidance of bloodstream infections. In this retrospective database analysis, the authors concluded that a potential savings of $773 per patient may be realized. Similarly, Pichard et al8 showed that 3-compartment PN bags were less expensive than hospital-compounded bag systems in terms of application costs. The authors concluded that the application cost of hospital-compounded bags was 150% of the 3-compatment bags. Manpower costs in hospital-compounded and 3-compartment bag systems were 15 CHF (Swiss Francs) and 10 CHF, respectively. The ratio of manpower costs was the same in both groups; they were 10% of total costs. Hospital-compounded bags are thought to be “tailor-made” and, therefore, to meet the patients’ specific requierements. However, it is estimated that a significant part of adult patients receiving PN in hospitals can be maintained with standard formulations that are provided by the industry.8 Furthermore, premixed multichamber bags have advantages, like prolongation of shelf life, reduction of personnel workload, and preclusion of admixing errors.9 Therefore, health care institutions should select the most effective way of providing PN while considering their specific circumstances. The decision whether to prepare PN admixtures internally or to purchase commercial products should be based on the type and size of a given hospital.10-12 Safety, economic, and ergonomic aspects are all factors that should be taken into consideration while administering PN in a given hospital.13,14
This retrospective observational study has some limitations. First, an actual cost comparison of the present study would have provided us with more realistic data, if this hospital had been using the 2 systems simultaneously. Unfortunately hospital-compounded and industrial multichamber bags cannot be routinely used simultaneously in most hospitals. In our center, only compounded bags have been used, and the final cost analysis may remain suppositional. Second, this retrospective analysis did not take the PN-related complications into account, which might have more realistically reflected the real-world situation. Finally, the results of the present study might be different if an alternative admixing system had been used. Automix 3+3 compounding system is relatively more economical compared to some other systems that require more transfer sets.
In concluson, this study shows a cost benefit of compounded PN compared to industrial multichamber bags, if more than 15 bags per day are used. In low-volume hospitals, industrial multichamber bags may be more advantageous.
Acknowledgments
We would like to thank the Nutrition Support Team at Hacettepe University Hospital and the teaching staff of the MBA Department of İstanbul Bilgi University. Also, we wish to thank Lila J. Lande, MPH, for her editing assistance.
References
- Pichard C, Schwarz G, Frei A, et al. Economic investigation of the use of three-compartment total parenteral nutrition bag: Prospective randomized unblinded controlled study. Clin Nutr. 2000; 4:245-251.
- Mühlebach S. Practical aspects of multichamber bags for total parenteral nutrition. Curr Opin Clin Nutr Metab Care. 2005;8:291-295.
- Wonka FE. Case study: Improved efficiency and reduced costs with premixed parenteral nutrition. Pharm Purch Prod. 2008;April:20-21.
- The United States Pharmacopeia and The National Formulary. Rockville, MD: US Pharmacopeial Convention Inc; 2008.
- Genton L, Mühlebach S, Dupertuis YM, Pichard C. Ergonomic and economic aspects of total parenteral nutrition. Curr Opin Clin Nutr Metab Care. 2006;9:149-154.
- Walter E, Liu FX, Matson P, et al. Cost analysis of neonatal and pediatric parenteral nutrition in Europe: A multi-country study [published online ahead of print]. Eur J Clin Nutr. doi: 10.1038/ejcl 2011.225.
- Turpin R, Canada T, Rosenthal V, et al. Bloodstream infections associated with parenteral nutrition preparation methods in the United States: A retrospective, large database analysis. J Parenter Enteral Nutr. 2012;36:169-176.
- Pichard C, Mühlebach S, Maisonneuve N, Sierro C. Prospective survey of parenteral nutrition in Switzerland: A three-year nationwide survey. Clin Nutr. 2001;20:345-350.
- Menne R, Adolph M, Brock E, Schneider H, Senkal M. Cost analysis of parenteral nutrition regimes in the intensive care unit: Three-compartment bag system vs multibottle system. J Parenter Enteral Nutr. 2008;32:606-612.
- Petrelli MD. Total parenteral nutrition: Economic investigations comparing hospital prepared nutritional bags versus similar bags prepared by the pharmaceutical industry. Rivista Italiana di Nutrizione Parenterale ed Enterale. 2004;22:186-192.
- Puntis J. Safe parenteral nutrition and the role of standardised feeds. Signa Vitae. 2010;5:8-12.
- Kochevar M, Guenter P, Holcombe B, Malone A, Mirtallo J; A.S.P.E.N. Board of Directors and Task Force on Parenteral Nutrition Standardization. A.S.P.E.N statement on parenteral nutrition standardization. J Parenter Enteral Nutr. 2007;31:
441-448. - Miller SJ. Commercial premixed parenteral nutrition: Is it right for your institution? Nutr Clin Pract. 2009;24:459-469.
- Bischoff SC. Organisation, regulation, preparation and logistics of parenteral nutrition in hospitals and homes: The role of the nutrition support team – Guidelines on Parenteral Nutrition, Chapter 8. Ger Med Sci. 2009;7:Doc20.

*Institute of Social Sciences, İstanbul Bilgi University, Istanbul, Turkey; †Eczacibasi-Baxter, Istanbul, Turkey; ‡Hospital Pharmacy, §Nutrition Support Team, ¶Department of General Surgery, Hacettepe University Teaching Hospital, Ankara, Turkey. Corresponding author: Erkut Bozat, Eczacibasi-Baxter, 2. cad. 1282. sok., Yukarı Ovecler, 06460, Ankara, Turkey; phone: +(90.533) 282 94 28; e-mail: erkutbozat@gmail.com