1Department of General Medicine, The Ipswich Hospital, Ipswich, United Kingdom; 2Department of Radiology, Barking, Havering and Redbridge NHS Trust, Romford, Essex, United Kingdom
Bifid ureters are a common malformation of the urinary system. In clinical practice, hydronephrosis resulting from obstruction of such a system is rare. The authors present a case involving an 88-year-old man admitted to the hospital with symptoms of renal failure, where bifid ureters were found incidentally in a hydronephrotic kidney during an emergency nephrostomy. This had been missed on a previous CT scan, resulting in a unique therapeutic dilemma.
• In symptomatic patients, bifid ureteric systems are often found to be dilated as a consequence of blind-ending branches and have frequently been described in medical literature; however, the finding of hydronephrosis resulting from tumor obstructing the bifid ureter is relatively rare.
• In clinical practice, it has been found that duplicated collecting systems are two times more common in women than men. In a recent study, approximately 11% of women were found to have duplicated systems compared with 5% of men.
• The formation of such ureteric systems can be explained by developmental errors during the early embryonic period, when the ureteric bud penetrates the metanephric tissue before splitting to form the renal pelvis and subsequently, the calyces. Duplicated systems arise as a consequence of early splitting of the bud or due to the development of two separate buds.
• The most common complication of a duplicated collecting system is reflux. The exact nature depends on the type of system involved. Complete systems are usually associated with vesicoureteric reflux.
• Although a traditional proximal approach was used in this case study, it could have performed by entering the ureter distally. This would have enabled the placement of a suitable Y-stent at the point where the two proximal branches met. However, because these cases are rare, the feasibility of such an approach needs further evaluation.
In 1948, Nordmark described bifid ureters, along with bifid renal pelves, as the most common malformation of the urinary system. Later studies confirmed this, with duplicated ureters being found in 1 in 125 patients (0.8%) in whom postmortem examinations were carried out.1,2 Often, these remain asymptomatic, and as a result, undiagnosed. In symptomatic patients, bifid ureteric systems are often found to be dilated as a consequence of blind-ending branches. Such cases have frequently been described in medical literature; however, the finding of hydronephrosis resulting from tumor obstructing the bifid ureter is relatively rare.
We present a case report of hydronephrosis due to back pressure from obstruction of the ureteric orifice. The obstruction resulted in dilatation of both the moieties of the bifid ureters, causing both a diagnostic and treatment dilemma.
Case Report
An 88-year-old man with stage IV chronic kidney disease was admitted with a complaint of generally feeling unwell associated with appetite and weight loss.
Chronic renal failure was presumed to be secondary to chronic interstitial nephritis due to long-term nonsteroidal anti-inflammatory drug use for rheumatoid arthritis for 30 years. The patient was also known to suffer from transitional cell carcinoma of the bladder, for which he had undergone a transurethral resection of bladder tumor. Magnetic resonance imaging (MRI) had shown two cortical lesions in the right kidney, one of which most likely represented renal cell carcinoma. Several Bosniak Type 1 cysts were also seen bilaterally. A repeat MRI performed 6 months after the initial one showed no significant change in lesion size.
The patient presented to the Accident and Emergency department at Queens with a week-long history of feeling generally unwell with associated complaints of loss of appetite, weight loss, and generalized pruritis. On admission, his renal function tests were urea 31.2 mmol/L, creatinine 367 μmol/L (baseline 280 μmol/L). Urine dipstick showed the presence of nitrites with a trace of leukocytes. Antibiotics and fluids were commenced and the patient was subsequently transferred to the medical ward under the care of the renal physicians.
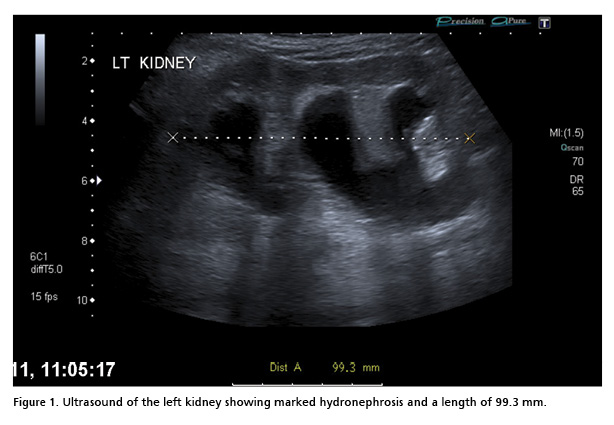
Due to the acute deterioration in the patient’s renal function, an ultrasound of the kidneys, ureters, and bladder was arranged in order to rule out a postrenal cause. The scan showed hydronephrosis of the left kidney, with a pelvic transverse diameter of 21 mm. The bladder was noted to be empty and there was no hydronephrosis seen in the right kidney.
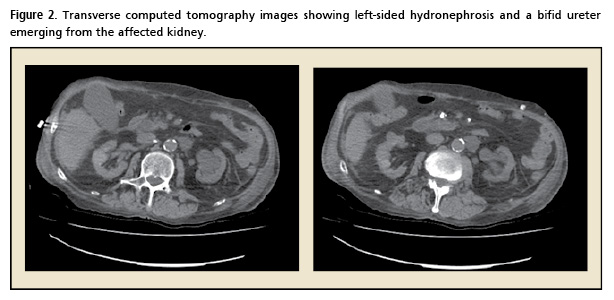
A subsequent computed tomography (CT; without contrast) showed diffuse wall thickening of the urinary bladder. The left ureteric orifice was also involved. According to the reporting radiologist, “back pressure changes” were observed in the affected ureter, and the hydronephrotic changes in the left kidney were easy to see on the images obtained. Due to the noncontrast nature of the CT scan, bifid ureters were missed by the reporting radiologist. Based on the diagnosis of hydronephrosis, a decision was made to perform a left-sided nephrostomy with stenting in order to aid recovery.
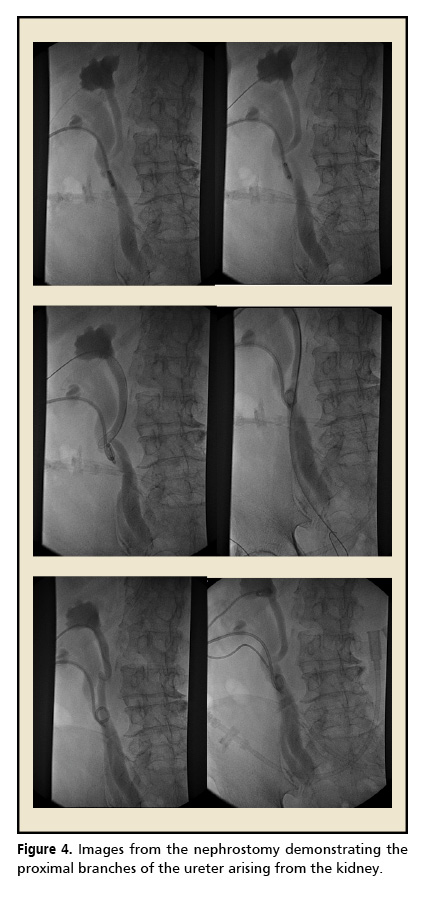
During the nephrostomy, the bifid ureter that had earlier been missed on the CT scan was identified. Stents were placed in both branches (8 Fr Skater in the upper ureter and 6 Fr Skater in the lower ureter). There were no immediate complications following the procedure and hemostasis was achieved successfully.
Unfortunately, the patient’s condition soon deteriorated and he died. Blood cultures taken during his hospital admission subsequently isolated gram-negative rods, confirming a diagnosis of urosepsis.
Discussion
In urology, duplicated collecting systems are kidneys with two pelvicaliceal systems. According to the nomenclature established by The Committee on Terminology, Nomenclature, and Classification of the Section on Urology of the American Academy of Pediatrics, these may be subdivided into partial or complete.3
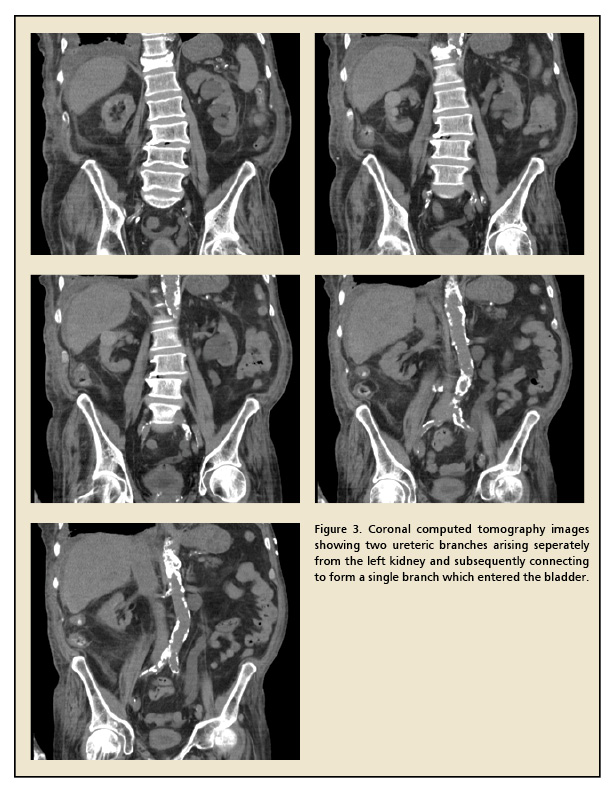
Bifid ureters fall into the first category, and may be defined as duplicated systems where two proximal branches drain the same pelvis, but join together distally to form one common ureteric branch prior to emptying into the bladder. However, complete duplicated systems are those where two ureters arise from the same kidney and drain separately into the bladder. Based on data published by Dahnert using urograms, partially duplicated systems are three times more common than complete ones.4 Similar findings were obtained by Prakash and colleagues in a recent study involving the use of intravenous pyelograms in 50 cadavers. Partially duplicated systems were found in three subjects, whereas complete duplication was present in one subject.5
In clinical practice, it has been found that duplicated collecting systems are two times more common in women compared with men. Data obtained recently using a study population of 774 children aged < 6 years with a history of urinary tract infections confirmed this. Approximately 11% of girls in the study were found to have duplicated systems compared with 5% of boys. In addition, of the 63 children with duplicated systems, 19% had them bilaterally.6 These results are comparable with those obtained by Whitaker and Danks who found unilateral duplication to be six times more common than bilateral duplication. It was also found that there was a one in eight possibility that a child with duplicated ureters would have a parent or sibling who was similarly affected.7
The formation of such ureteric systems can be explained by developmental errors during the early embryonic period, when the ureteric bud penetrates the metanephric tissue before splitting to form the renal pelvis and subsequently, the calyces. Duplicated systems arise as a consequence of early splitting of the bud or due to the development of two separate buds.
The most common complication of a duplicated collecting system is reflux. The exact nature depends on the type of system involved. Complete systems are usually associated with vesicoureteric reflux. This tends to affect the lower pole which is usually laterally positioned in the bladder according to the Weigert-Myer law.8 Bisset and Strife found that the incidence of reflux associated with complete duplicated systems was 69%,9 which is comparable with that found by Fehrenbaker and colleagues (72%).10 The lower pole was much more commonly affected. On the other hand, reflux associated with partially duplicated systems tends to by ureteroureteric. The incidence of reflux found by Bisset and Strife in partially duplicated systems (22%) was similar to that found in individuals with nonduplicated systems.9
Blind-ending branches of bifid ureteric systems have often been described in the medical literature. Ureteroureteric or uterterorenal reflux may occur, resulting in dilatation of the collecting system. This may result in hydronephrosis. However, cases involving hydronephrosis occurring in spite of both branches being initially patent are, to our knowledge, rare. Though Megremis and associates recently described a case involving simultaneous obstruction of both branches of a bifid system by calculi,11 there was no evidence of hydronephrosis (the upper ureters were mildly dilated) and treatment involved extracorporeal shockwave lithotripsy. The case just described involved hydronephrosis severe enough to warrant a nephrostomy.
As the bifid ureter had not been previously detected on imaging, it posed an interesting therapeutic dilemma when it was eventually found during the nephrostomy. Though the procedure was performed using the traditional proximal approach, an argument could have been made for it to be performed by entering the ureter distally. This would enable the placement of a suitable Y-stent at the point where the two proximal branches met. However, as cases such as this are rare, the feasibility of such an approach needs further evaluation.
References
Nation EF. Duplication of the kidney and ureter: a statistical study of 230 new cases. J Urol. 1944; 51:456-465.
Campbell MF. Anomalies of the ureter. In: Campbell MF, Harrison JH, eds. Urology, 3rd ed. Philadelphia: WB Saunders; 1970:1487-1670.
Glassberg KI, Braren V, Duckett JW, et al. Suggested terminology for duplex systems, ectopic ureters and ureteroceles. J Urol. 1984;132:1153-1154.
Dahnert W. Radiology Review Manual, 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
Prakash RT, Venkatiah J, Bhardwaj AK, et al Double ureter and duplex system: a cadaver and radiological study. JUrol. 2011;8:145-148.
Siomou E, Papadopoulou F, Kollios KD, et al. Duplex collecting system diagnosed during the first 6 years of life after a first urinary tract infection: a study of 63 children. J Urol. 2006;175:678-681; discussion 681-682.
Whitaker J, Danks DM. A study of the inheritance of duplication of the kidneys and ureters. J Urol. 1966;95:176-178.
Decter RM. Renal duplication and fusion anomalies. Pediatr Clin North Am. 1997;44:1323-1341.
Bisset GS 3rd, Strife JL. The duplex collecting system in girls with urinary tract infection: prevalence and significance. AJR Am J Roentgenol. 1987;148:497-500.
Fehrenbaker LG, Kelalis PP, Stickler GB. Vesicoureteral reflux and ureteral duplication in children. J Urol. 1972;107:862-864.
Megremis S, Chatziioannou M, Tritou I. Simultaneous obstruction of both limbs of a bifid ureter by calculi. J Ultrasound Med. 2010;29:145-147.