Department of Urology, Bhopal Memorial Hospital and Research Centre, Bhopal, India
We recently cared for a patient with adenocarcinoma of the pancreas who presented with ureteral metastasis followed by hydroureteronephrosis long before the appearance of any symptoms related to the primary lesion. The entity is extremely rare; only seven similar cases are on record in the scientific literature. No recent review exists on this topic. This encouraged us to present our case along with the previous cases of adenocarcinoma of the pancreas with ureteral metastasis that have been reported.
Among half of the cases, the breast or gastrointestinal tract (colorectum) is the site for primary cancer. Prostate cancer and uterine cervical cancer are responsible for 30% to 40% of cases, with stomach and lung cancer being reported in the remaining cases.
Among half of the cases, the breast or gastrointestinal tract (colorectum) is the site for primary cancer. Prostate cancer and uterine cervical cancer are responsible for 30% to 40% of cases, with stomach and lung cancer being reported in the remaining cases.
The ureters do not possess a continuous longitudinal network of blood and lymph vessels inside their walls (intramural); thus, they are relatively resistant to metastatic rests of tumor cells by hematogenous and lymphatic routes, which are the two most common routes of metastasis of most primary malignancies.
Main Points
• Metastatic tumors of the ureter are uncommon, and one of the rarest causes of ureteric obstruction. The majority of ureteric metastatic cancers are asymptomatic and diagnosed at autopsy, or when metastatic involvement of other organs had occurred, which makes the diagnosis more obvious.
• Whenever symptomatic, this particular entity presents with nonspecific symptoms secondary to ureteric obstruction. Back pain occurs in approximately 50% of patients. Other symptomatology usually includes urinary tract infection, frequency, dysuria, proteinuria, and hematuria (incidence 20% to 30%, indicates mucosal involvement).
• Ureteral catheters or internal double-J stents are good treatment options for ureteral obstruction and are well tolerated. Nephrostomy or ureteric reimplantation is indicated when ureteral catheterization is not possible. Radiotherapy has been used but urinary diversion provides much more rapid relief.
• Although the prognosis is generally poor, whenever ureteral metastasis is suspected, early and aggressive workup followed by appropriate treatment of ureteral obstruction may preserve renal function and increase survival rate.
• The presence of ureteral metastases indicates advanced disease and the prognosis is bleak.
Although, ureteral obstruction is relatively common in patients with locally invasive pelvic malignancies, it is extremely rare to find ureteral obstruction due to metastases to the ureter from distant primary tumors.1-4 Only approximately 400 such cases have been reported.1,2 Most reported cases were diagnosed postmortem. Ureteral metastases from pancreatic adenocarcinoma have been reported in only seven published cases until now. In the case of the tumors in sites other than the pancreas with ureteral metastases, the primary lesions usually become evident before the ureteral lesions are found.5 Three of the seven (43%) reported cases of pancreatic adenocarcinoma presented with initial urologic complaints, and not with complaints related to the primary lesion. We report on a case of pancreatic adenocarcinoma that presented with ureteral metastasis and hydronephrosis. This case also had metastatic invasion of all layers of the ureter which is another infrequent and unique finding.3 We also review the seven previously reported cases here, along with the relevant literature.
Case Report
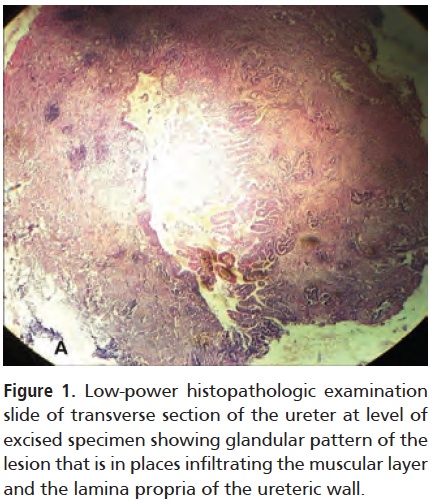
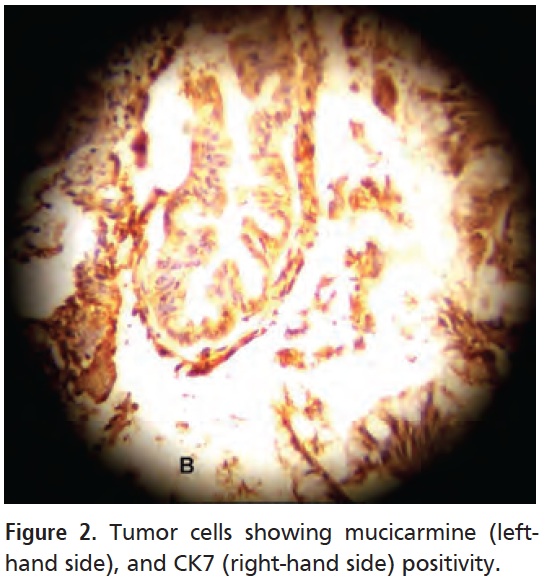
A 54-year-old man was referred to our center for right loin pain of 1.5 months’ duration. All laboratory parameters were normal. Ultrasonography (USG) revealed moderate right hydrouretronephrosis (HUN) and thinned out parenchyma of the right kidney. No calculus could be visualized. USG did not reveal any other abnormality. Intravenous urography showed compromised right renal function with lower ureteric obstruction. Computed tomography (CT) urography confirmed the findings of moderate HUN with lower ureteric block with no evidence of calculus or tumor in the ureter. Considering genitourinary tuberculosis (GUTB), which is common in the Indian subcontinent, and at the top of the list of differential diagnosis, the patient was provisionally diagnosed with GUTB and empirical antitubercular therapy was initiated. A per-cutaneous nephrostomy tube was inserted that started draining 800 to 900 mL of urine per 24 hours. A diethylene-triamine-penta-acetic acid renal scan was performed that revealed only 23% relative function of the right kidney and poor response to the diuretic. In view of his limited renal function, the patient was advised to undergo nephroureterectomy, but he did not consent. After several days, a nephrostogram was performed that revealed lower ureteric stricture. The patient was scheduled for a double-J stenting approximately 3 weeks later. Retrograde pyelogram performed at the start of the procedure showed a complete lower ureteric block, and the stent could not be inserted by either antegrade or retrograde technique. Thus, we planned ureteroneocystostomy by an extraperitoneal approach. Intraoperatively, a 3-cm segment of the lower right ureter was found to be hard in consistency. It was excised and sent for biopsy. We performed Boari flap-ureteroneocystostomy and inserted a double-J stent. Histopathologic examination (HPE) of the excised specimen revealed mucin-producing glandular structures that had infiltrated the muscular layer and the lamina propria of the ureter (Figure 1). The cells of the glands showed marked nuclear pleomorphism and a mild increase in mitoses. The tumor had also involved about two-thirds of the ureteral mucosa. Tumor cells were positive for mucicarmine and immunohistochemical stains including carcinoembryonic antigen, carbonic anhydrase 19.9, cytokeration (CK)7, and CK20 (Figure 2). Final diagnosis given by our pathologist was invasive mucinous adenocarcinoma of the ureter.
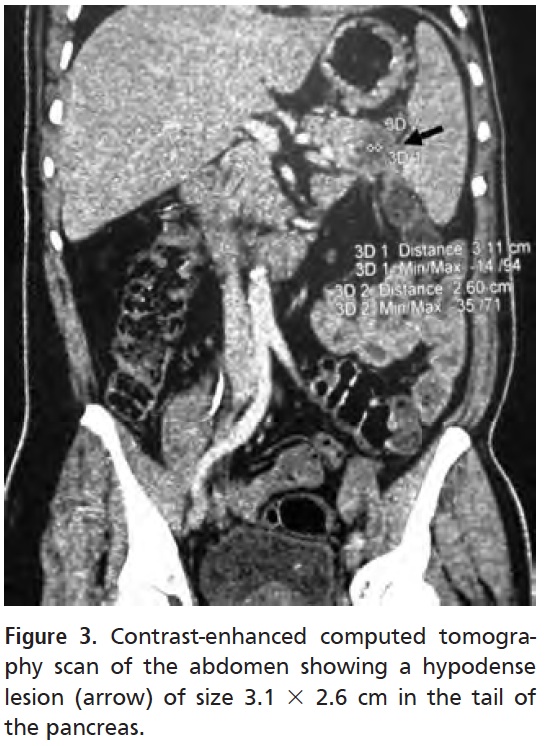
Once confirming the diagnosis of metastatic ureteral tumor in this patient, a search for the primary lesion was initiated immediately. Upper gastrointestinal endoscopy (UGIE) and colonoscopy did not reveal any abnormality. An earlier CT urography was reviewed. Because of some doubt during its review, a contrast-enhanced CT scan of the whole abdomen was performed that showed a hypodense lesion measuring 3.1 × 2.6 cm in the tail of the pancreas (Figure 3), and multiple subcentimetric size paraaortic and splenic hilar lymph nodes. CT-guided fine needle biopsy of the lesion revealed well-differentiated mucinous adenocarcinoma. As advised by the medical oncologist, the patient underwent gemcitabine-based chemotherapy. At 11-month follow-up, the pancreatic lesion had regressed in size.
Discussion
Metastatic tumors of the ureter are uncommon, and one of the rarest causes of ureteric obstruction.2,4 Since their first mention in the literature by Stow in 1909,6 only approximately 400 cases are on record in the literature.1,2 According to autopsy data, incidence of ureteral metastasis ranges anywhere from between 0.3% and 8.3%.7 MacLean and Fowler, in a series of 10,233 consecutive autopsies, found only 0.37% incidence of ureteral metastatic cancer.8 Cohen and colleagues9 found ureteral metastasis among 31 patients (0.96%) in a study of 3200 autopsies, 7 of whom had breast cancer. However, findings by Geller and Lin, of 181 patient autopsies who had been diagnosed with breast cancer,10 revealed that prevalence among this subgroup is much higher. The majority of ureteric metastatic cancers are asymptomatic.9,11 Most of the reported cases have been diagnosed based on autopsy findings, or when metastatic involvement of other organs had occurred and had made the diagnosis obvious.12 But the incidence of diagnosing ureteral metastasis in patients while they are living is exceedingly rare. However, the wide availability of radiographic testing has greatly increased the rate of incidental findings. Such findings raise physician awareness and alert them to perform a more aggressive workup. This may lead to a possible increase in the number of living cases with a diagnosis of ureteral metastases.
Among half of the cases, the breast or gastrointestinal tract (colorectum) is the site for primary cancer. Prostate cancer and uterine cervical cancer are responsible for 30% to 40% of cases, with stomach and lung cancer being reported in the remaining cases.9,11,13 The pancreas has been reported as the least likely site of primary cancer.9,14 Among 10,233 consecutive autopsies, MacLean and Fowlernoted only one case of adenocarcinoma of the pancreas with ureteric obstruction.8
Microinvolvement of the Ureter by Metastases and Its Mechanism
Involvement of the ureter by the metastases may occur as one of three different types.4,9,11,15,16
Type I: Periureteral adventitial layer involvement or infiltration by the tumor cells is the most common of all the three types. This involvement usually results in compression of the ureteral wall.
Type II: Involvement of a portion of the layers of the ureter or transmural involvement along with presence of tumor cells in the muscular coat, perilymphatic, and/or vascular layers of the ureter.
Type III: The involvement of local mucosa of the ureter with or without muscularis layer, and submucosal nodules, is the most uncommon.
As the periureteral adventitial soft tissue is longitudinal, blood vessels are very well developed in this layer. This may be why hematogenous metastases occur more often in the periureteral tissue, and it is this periureteral tissue layer of the ureter that is usually first involved in metastases to the ureter.17,18 Furthermore, periureteral adventitial infiltration occurs because of deposition of tumor cells in the longitudinal blood vessels, which then start growing perpendicular to the long axis of the ureter.17 Muscularis and mucosa of the ureter, on the other hand, are supplied smaller arteriols that are running perpendicular to the length of the ureter.9,15-17,19; Thus, the involvement of muscularis and lamina propria occurs as a result of direct extension or along vascular channels. In addition, although rare, attenuation or ulceration of the mucosa may eventually occur.18 Transmural metastases occur due to deposition of tumor cells within the muscularis followed by circumferential spread leading to stricture formation of the involved segment of the ureter.The mechanism of formation of submucosal nodules with or without mucosal invasion is transportation of implanted tumor cells (that get shed into the urine) to the lamina properia by perforating arteriols.17
The ureters do not possess a continuous longitudinal network of blood and lymph vessels inside their walls (intramural); thus, they are relatively resistant to metastatic rests of tumor cells by hematogenous and lymphatic routes,20 which are the two most common routes of metastasis of most primary malignancies. Furthermore, the flow of lymph in the lower ureter is downward, whereas that in the pelvic organs flows in the opposite direction. This creates a counter-current effect and thus may act as a barrier against metastatic deposition of tumor cells in the ureteric wall.21
Type I and Type II metastatic ureteral involvement result in stricture formation, or even obstruction of the ureter with or without associated mass. Type III may manifest as filling defects within the ureteral lumen seen radiographically.22
Ureteral metastasis may involve any portion of the ureter 23 and bilateral involvement occurs in approximately 25% to 70% of cases.14,24 Periureteral layer involvement is more common than transmural and submucosal nodules with mucosal involvement, and this term has been used interchangeably with ureteral metastasis.20 Our case is unique in that there was an actual invasion of all the three layers of the ureteric wall (which is extremely unusual).3
Criteria for Diagnosis
It is important and difficult to differentiate between primary and secondary tumors of the ureter. Criteria for actual ureteral metastasis were first developed by MacKenzie and Ratner in 1931.21 They noted that, in cases of metastatic tumors of the ureter, the perivascular lymphatic spaces or the blood vessels around the ureter would always show malignant cells.21 These criteria were later modified by Presman and Ehrlich20 who stated that “demonstration of malignant cells in a portion of the ureteral wall along with the absence of any neoplasm in adjacent tissues” is the most important finding in favor of ureteral metastasis.25 This means that true metastases grow within the ureteral wall and/or within the immediate periureteral lymphatics or tissues without any involvement of the ureter by direct extension.26
Clinical Picture
Many cases of ureteral metastases that have been reported thus far have been asymptomatic and were found incidentally at autopsy.9,11,14 Whenever symptomatic, this particular entity presents with nonspecific symptoms secondary to ureteric obstruction. Back pain occurs in approximately 50% of patients. Other symptomatology usually includes urinary tract infection (UTI), frequency, dysuria, proteinuria, and hematuria (incidence 20% to 30%, indicates mucosal involvement).9,14 UTI is a common accompaniment and usually manifests as frequency. Anuria is rare but may occur with bilateral involvement27;however, as many as 50% of patients are expected to have impaired renal function at the time of admission.28 Although ureteral obstruction/urologic symptoms usually manifest within 1 year of the detection of the primary cancer, rarely do these present as the first indication of metastasis,4,29 and most patients will have extensive metastasis to other organs at the time ureteral involvement is discovered.20
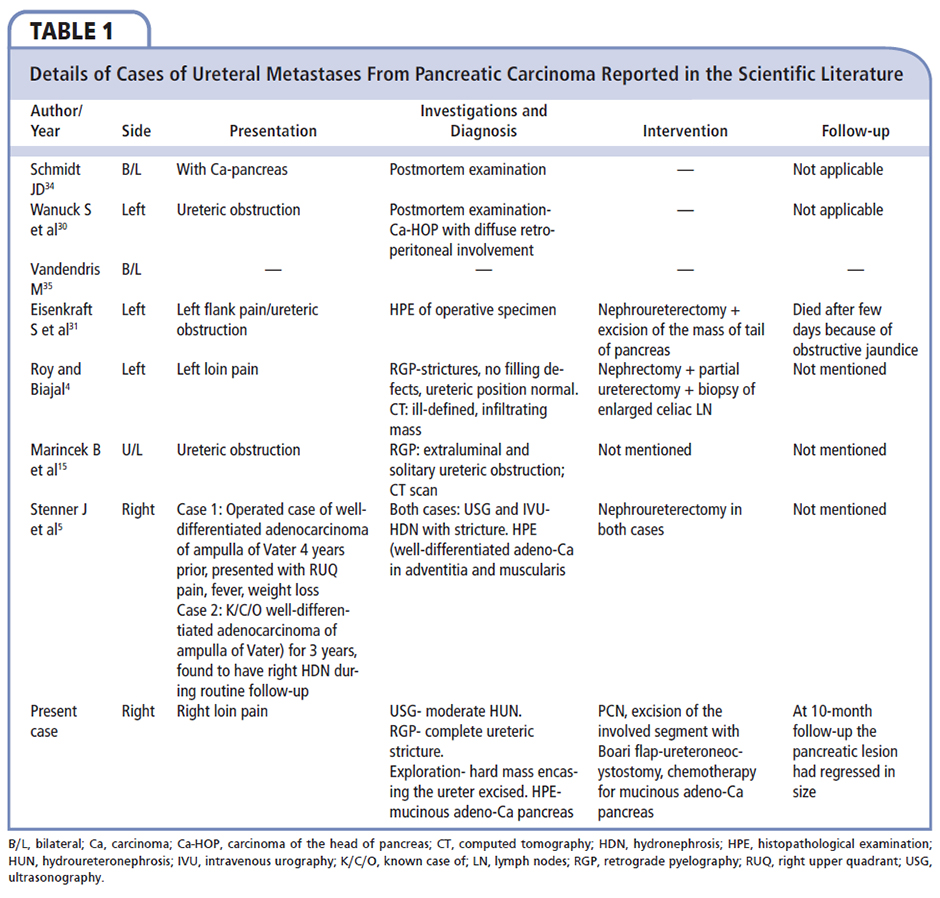
Table 1 lists the details of the reported cases of ureteral metastasis from pancreatic carcinoma in the scientific literature. Wanuck and colleagues30 reported on a case of carcinoma of the head of pancreas (Ca-HOP) that presented as ureteric obstruction, but the actual culprit disease was only discovered at autopsy because the ureteral involvement simulated the primary ureteral tumor. Here lies the importance of the need to differentiate between the latter and the ureteral metastases. However, most likely the case reported by Wanuck and associates30 and that by Eisenkraft and colleagues31 did not represent true ureteral metastases but only direct extension of the pancreatic cancer. Autopsy findings of the case reported by Wanuck and associates30 had revealed that it was actually Ca-HOP with diffuse retroperitoneal involvement leading to ureteric obstruction. Likewise, in the case reported by Eisenkraft and colleagues,31 exploration of kidney, ureter, and bladder region revealed a retroperitoneal tumor that had encased the left ureter and renal pelvis. Autopsy revealed that it was actually due to primary anaplastic carcinoma of the pancreatic tail with retroperitoneal involvement and resultant blockade of the left ureter.31 Therefore, these two cases might have had retroperitoneal metastases from pancreatic cancer, which is uncommon but cannot be considered invasive metastases of the ureter itself. Ureteral wall invasion as such is even more uncommon.
Mechanism of Obstruction
Ureteral metastatic tumors usually lead to mechanical ureteral obstruction. Different mechanisms cited in this regard include encasement and concentric occlusion of the ureter by the metastatic tumor deposits, direct extrinsic pressure, vigorous fibroblastic/sclerosing reaction leading to stricture formation, fibrosis with traction on a segment of the ureter resulting in obstructive angulation, or even invagination of the upper ureteral segment into the lower portion.7,9,19 Interference with nerve and blood supply, as well as edema, causes reduced peristaltic activity and resulting hydroureter.7
Work-up
The findings of thickening and/or stenosis of the ureteral wall, or HUN, can be easily detected on radiography. Contrast studies reveal the site of stricture with HUN and displaced ureter. Ureteric mucosa is typically intact.4,32 However, there are many causes of ureteric stricture, including inflammation and neoplasticity, that can have similar radiographic features. Roy and Biajal published a good review on differential diagnosis of ureteric strictures, and provided a simple and useful diagnostic algorithm for cases presenting with ureteric obstruction.4 Although the most common causes can be ruled out on the basis of history and clinical picture (eg, iatrogenic, those due to passage of stone, postradiation stricture, traumatic, tuberculosis) along with local examination (eg, ureteral obstruction in colon, prostate, and cervical cancers, and endometriosis),HPE confirmation is necessary for the diagnosis of ureteral metastases.4 CT scan provides the most significant details of the retroperitoneum in such cases and is extremely helpful, therefore, CT of the entire abdomen should be performed. Any mass lesion at a remote site from the diseased ureter site would be an important diagnostic point in favor of ureteral metastases, andshould be biopsied for confirmation by HPE.4 Problems arise when the primary lesion is occult. A high degree of suspicion needs to be maintained in such situations. Screening for primary lesions should include stool examination for occult blood, UGIE, colonoscopy (and biopsy), mammography, and breast USG.
As the two most common patterns of involvement in ureteral metastasis are extramucosal, ureteroscopic biopsy is less useful. Luciani and colleagues used fine-needle aspiration cytology performed under fluoroscopic guidance to establish the true nature of ureteral stenosis in 15 patients with known primary malignancy, which had previously been treated with surgery, radiotherapy, or chemotherapy.They found the technique to be 80% successful (with 100% accuracy) in differentiating ureteral metastases from postradiation fibrosis.33
Although desmoplastic reaction can occur with any tumor and can lead to prominent fibrous tissue formation around malignant cells, it is highly provoked by metastases from tumors with scirrhous growth (prostate, stomach, colon).15 Thus, ureteral wall thickening seen on CT scan is a nonspecific finding.22 It is difficult to differentiate between metastasis and primary urothelial tumors on CT. Metastatic lesions show focal circumferential thickening of the ureter (involvement of transmural involvement of the ureteral wall) that may be associated with ill-defined extraluminal soft tissue (infiltration of the periureteric soft tissue) masses.17
Treatment
Ureteral obstruction must be relieved.17,18 Ureteral catheters or internal double-J stents are good options and are well tolerated, and may be left in place for long periods if necessary.17 Nephrostomy or, in some cases, ureteric reimplantation is indicated when ureteral catheterization is not possible. Nephrectomy is only rarely required.
Radiotherapy has been used27 but urinary diversion provides much more rapid relief. Most patients will have other evidence of metastatic disease and systemic therapy is required. Systemic therapy in this situation is identical to that for metastatic primary cancer.
Prognosis
Approximately 90% of patients with ureteral metastasis has evidence of metastatic disease20 and, when found, is almost always indicative of advanced metastatic disease.24 Although the prognosis is generally poor, with75% of patients dying within 6 months after onset of symptoms of ureteral obstruction,2 whenever ureteral metastasis is suspected, early and aggressive workup followed by appropriate treatment may preserve renal function and increase the survival rate. This may be especially important in patients who do not have significant clinical symptoms or those who have developed ureteral metastases after a positive response to chemotherapy has occurred.
Conclusions
Ureteral metastases are very rare but must be kept in the differential diagnosis when a patient who has malignant disease has evidence of ureteral obstruction on radiographic studies. The presence of ureteral metastases indicates advanced disease and the prognosis is bleak.
References
Haddad FS. Metastases to the ureter. Review of world literature, and three new case reports. J Med Liban. 1999;47:265-271.
Katsuno G, Kagawa S, Kokudo Y, et al. Ureteral metastasis from appendiceal cancer: report of a case. Surg Today. 2005;35:168-171.
Goel AK, Rao MS, Mathur RP, et al. Bilateral ureteric and renal pelvic invasion by metastatic oesophageal carcinoma (a case report). J Postgrad Med. 1985;31:212-214.
Roy S, Baijal SS. Pancreatic adenocarcinoma presenting with ureteric metastases. Case report and review of literature. Clin Imaging. 1993;17:99-103.
Stenner J, Arista-Nasr J, Leñero-Llaca E, et al. Adenocarcinoma of the ampulla of Vater and head of the pancreas metastatic to the ureter: report of 2 cases. J Urol. 1996;156:1765.
Stow B. Fibrolymphosarcomata of both ureters metastatic to a primary lymphosarcoma of the anterior mediastinum of thymus origin. Ann Surg. 1909;50:901-906.
Talreja D, Opfell RW. Ureteral metastasis in carcinoma of the breast. West J Med. 1980;133:252-254.
MacLean JT, Fowler VB. Pathology of tumors of the renal pelvis and ureter. J Urol. 1956;75:384-415.
Cohen WM, Freed SZ, Hasson J. Metastatic cancer to the ureter: a review of the literature and case presentations. J Urol. 1974;112:188-189.
Geller SA, Lin C. Ureteral obstruction from metastatic breast carcinoma. Arch Pathol. 1975;99:476-478.
Marincek B, Scheidegger JR, Studer UE, Kraft R. Metastatic disease of the ureter: patterns of tumor spread and radiologic findings. Abdom Imaging. 1993;18:88-94.
Fitch WP, Robinson JR, Radwin HM. Metastatic carcinoma of the ureter. Arch Surg. 1976;111:874-876.
Witten D, Myers GH Jr, Utz DC, Eds. Emmett’s Clinical Urography: An Atlas and Textbook of Roentgenologic Diagnosis, 4th ed. Philadelphia: WB Saunders; 1977.
Stearns DB, Gordon SK. Ureteral metastasis secondary to carcinoma of the large bowel. Am J Surg. 1960;99:244-246.
Alexander S, Kim K, Pinck BD, Brendler H. Metastatic ureteral tumors. J Urol. 1973;110:288-290.
Presman D, Ehrlich L. Metastatic tumors of the ureter. J Urol. 1948;59:312-325.
Mackenzie DW, Ratner M. Metastatic growths of the ureter: a report of three cases and a brief review of the literature. Can Med Assoc J.1931;25:265-270.
Bechtold RB, Chen MY, Dyer RB, Zagoria RJ. CT of the ureteral wall. Am J Roentgenol. 1998;170:1283-1289.
Grabstald H, Kaufman R. Hydronephrosis secondary to ureteral obstruction by metastatic breast cancer. J Urol. 1969;102:569-576.
Babaian RJ, Johnson DE, Ayala AG, Sie ET. Secondary tumors of the ureter. Urology. 1979;14:341-343.
Shimoyama Y, Ohashi M, Hashiyuchi N, et al. Gastric cancer recognized by metastasis to the ureter. Gastric Cancer. 2000;3:102-105.
Benejam R, Carroll TJ, Loening S. Prostate carcinoma metastatic to ureter. Urology. 1987;29:325-327.
Puech JL, Song MY, Joffre F, et al. Ureteral metastases—computed tomographic findings. Eur J Radiol. 1987;7:103-106.
Ambos MA, Bosniak MA, Megibow AJ, Raghavendra B. Ureteral involvement by metastatic disease. Urol Radio1. 1979;l:105-112.
Giuliano AE, Sparks FC, Morton DL. Breast cancer presenting as renal colic. Am J Surg. 1978;135:842-845.
Wanuck S, Schwimmer R, Orkin L. Carcinoma of the pancreas causing ureteral obstruction. J Urol. 1973;110:395-396.
Eisenkraft S, Jonas P, Mani M. Left nephroureteric obstruction due to carcinoma of the pancreatic tail. Br J Urol. 1986;58:97-98.
Goldman SM, Gatewood OMB. Neoplasms of the renal collecting system, pelvis, and ureter. In: Pollack HM, ed. Clinical Urography. An Atlas and Textbook of Urologic Imaging. Philadelphia: W.B. Saunders; 1999:1339-1349.
Luciani L, Scappini P, Pusiol T, Piscioli F. The role of aspiration cytology in the management of ureteral obstruction in patients with known cancer.Cancer. 1987;59:1936-1946.
Schmidt JD. Bilateral ureteral obstruction due to cancer of the pancreas. J Urol. 1971;106:652-654.
Vandendris M. Complete bilateral ureteral obstruction secondary to pancreatic carcinoma. Eur Urol. 1976;2:43-44.