Anomalous Origin of the Right Coronary Artery From the Left Anterior Descending Artery With Anomalous Course Between the Great Vessels: A Case for Conservative Management With Review of the Literature
Prakash Suryanarayana, MD,1 Shubha Kollampare, MD,2 Mohammad Reza Movahed, MD1,3
1Department of Medicine, Division of Cardiology, University of Arizona School of Medicine, Tucson, AZ;
2Department of Medicine, University of Arizona School of Medicine, Tucson, AZ;
3CareMore Arizona, Tucson, AZ
A single left coronary artery is a rare coronary anomaly. In such situations, the right coronary artery arises from the left anterior descending artery and traverses an unusual proximal course between the aorta and pulmonary trunk. There are only 10 such reported cases in the medical literature to date. After a detailed risk-to-benefit consideration, the decision was made for conservative management. In this report, we describe this rare case with a detailed review of the literature.
[Rev Cardiovasc Med. 2015;16(3):221-224 doi: 10.3909/ricm0774]
© 2015 MedReviews®, LLC
Anomalous Origin of the Right Coronary Artery From the Left Anterior Descending Artery With Anomalous Course Between the Great Vessels: A Case for Conservative Management With Review of the Literature
Prakash Suryanarayana, MD,1 Shubha Kollampare, MD,2 Mohammad Reza Movahed, MD1,3
1Department of Medicine, Division of Cardiology, University of Arizona School of Medicine, Tucson, AZ;
2Department of Medicine, University of Arizona School of Medicine, Tucson, AZ;
3CareMore Arizona, Tucson, AZ
A single left coronary artery is a rare coronary anomaly. In such situations, the right coronary artery arises from the left anterior descending artery and traverses an unusual proximal course between the aorta and pulmonary trunk. There are only 10 such reported cases in the medical literature to date. After a detailed risk-to-benefit consideration, the decision was made for conservative management. In this report, we describe this rare case with a detailed review of the literature.
[Rev Cardiovasc Med. 2015;16(3):221-224 doi: 10.3909/ricm0774]
© 2015 MedReviews®, LLC
Anomalous Origin of the Right Coronary Artery From the Left Anterior Descending Artery With Anomalous Course Between the Great Vessels: A Case for Conservative Management With Review of the Literature
Prakash Suryanarayana, MD,1 Shubha Kollampare, MD,2 Mohammad Reza Movahed, MD1,3
1Department of Medicine, Division of Cardiology, University of Arizona School of Medicine, Tucson, AZ;
2Department of Medicine, University of Arizona School of Medicine, Tucson, AZ;
3CareMore Arizona, Tucson, AZ
A single left coronary artery is a rare coronary anomaly. In such situations, the right coronary artery arises from the left anterior descending artery and traverses an unusual proximal course between the aorta and pulmonary trunk. There are only 10 such reported cases in the medical literature to date. After a detailed risk-to-benefit consideration, the decision was made for conservative management. In this report, we describe this rare case with a detailed review of the literature.
[Rev Cardiovasc Med. 2015;16(3):221-224 doi: 10.3909/ricm0774]
© 2015 MedReviews®, LLC
KEY WORDS
Anomalous coronary artery • Atherosclerosis • Coronary artery disease • Angina • Angiogram • Cardiac catheterization
KEY WORDS
Anomalous coronary artery • Atherosclerosis • Coronary artery disease • Angina • Angiogram • Cardiac catheterization
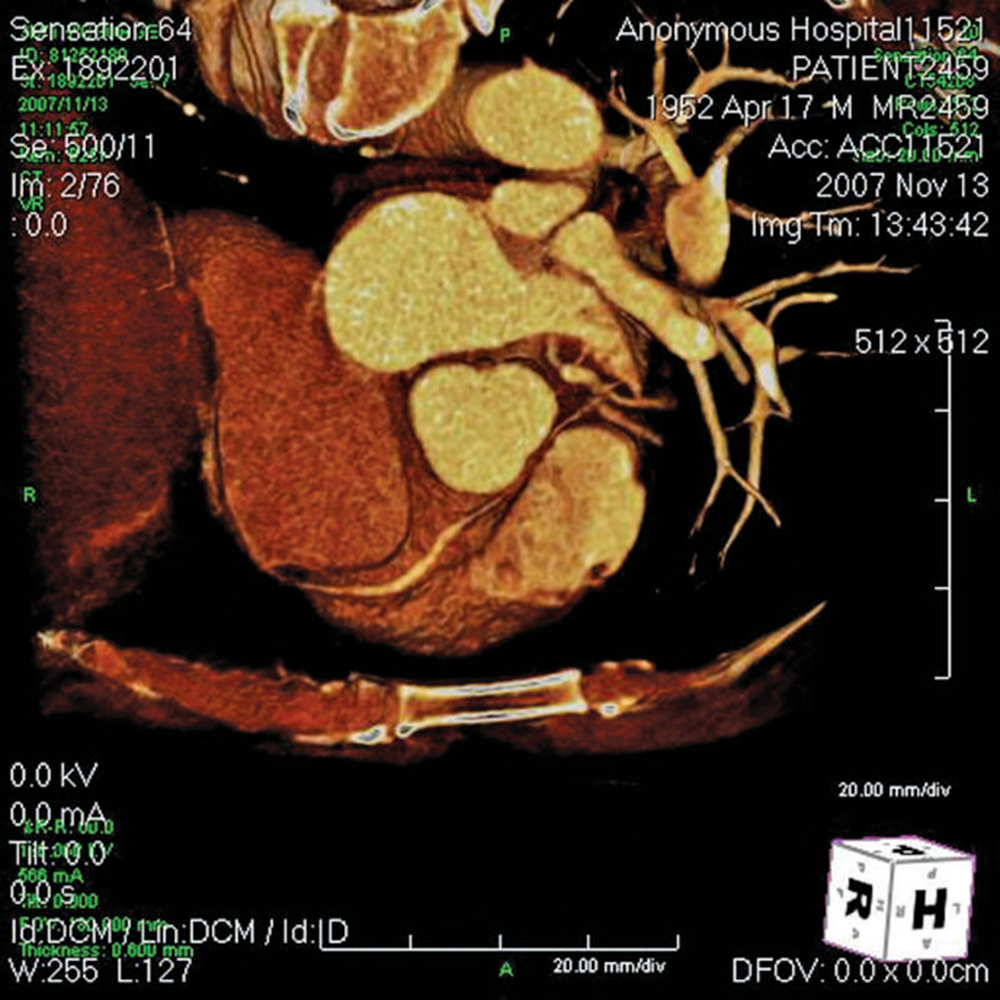
Figure 1. Anomalous right coronary artery (RCA) originating from the left anterior descending artery and passing between the aorta and the pulmonary trunk. Note the narrowed segment of the RCA as it courses between the two major vessels.
Cardiac computed tomography angiography … revealed a right dominant circulation with an anomalous RCA arising from the LAD, coursing between the aorta and pulmonary artery.
… anomalous coronary arteries originating from the contralateral aortic sinus coursing between the pulmonary artery and the aorta have received much attention because of their association with SCD.
Although survival after bypass may be better when an IM graft is used, it is prone to atrophy due to competitive flow within the native vessel.
Main Points
• A single left coronary artery is a rare coronary anomaly. In such situations, the right coronary artery (RCA) arises from the left anterior descending artery (LAD) and traverses an unusual proximal course between the aorta and pulmonary trunk. Most anomalies are asymptomatic and are seen as incidental findings on coronary angiography.
• Anomalous coronary arteries originating from the contralateral aortic sinus coursing between the pulmonary artery and the aorta have received much attention because of their association with sudden cardiac death. Many patients with that type of abnormality are asymptomatic before the fatal event. Thus, when these patients are identified, aggressive surgical management is often recommended.
• Various surgical options are available, including coronary bypass (with or without ligation of the anomalous vessel using an internal mammary or saphenous vein graft), coronary reimplantation, or unroofing procedures.
• Noticeable differences are seen in the presentation and clinical course among patients with anomalous left coronary artery (ALCA) and anomalous right coronary artery abnormalities; the majority of deaths have occurred in ALCA patients.
Main Points
• A single left coronary artery is a rare coronary anomaly. In such situations, the right coronary artery (RCA) arises from the left anterior descending artery (LAD) and traverses an unusual proximal course between the aorta and pulmonary trunk. Most anomalies are asymptomatic and are seen as incidental findings on coronary angiography.
• Anomalous coronary arteries originating from the contralateral aortic sinus coursing between the pulmonary artery and the aorta have received much attention because of their association with sudden cardiac death. Many patients with that type of abnormality are asymptomatic before the fatal event. Thus, when these patients are identified, aggressive surgical management is often recommended.
• Various surgical options are available, including coronary bypass (with or without ligation of the anomalous vessel using an internal mammary or saphenous vein graft), coronary reimplantation, or unroofing procedures.
• Noticeable differences are seen in the presentation and clinical course among patients with anomalous left coronary artery (ALCA) and anomalous right coronary artery abnormalities; the majority of deaths have occurred in ALCA patients.
A 55-year-old man presented with complaints of chest pain of 2 years' duration. The pain was brought on by exertion and relieved at rest. He had risk factors for coronary artery disease, including hypertension and hypercholesterolemia. He consumed approximately 2 to 3 glasses of vodka every night. He was given a stress test at another institution that was not indicative of inducible ischemia and revealed normal chronotropic competence. His home medications included amlodipine and aspirin. Results of physical examination and laboratory investigation were unremarkable. His electrocardiogram revealed normal sinus rhythm at a rate of 80 beats/min, left axis deviation, left atrial abnormality, and T-wave inversion in lead V6. Due to exertional chest pain suggestive of angina, he underwent cardiac catheterization, which revealed moderate left ventricular dysfunction with an ejection fraction of 30% to 35% and global hypokinesis. This was thought to be secondary to chronic alcoholism. Surprisingly, he also had an anomalous right coronary artery (RCA) originating from the left anterior descending artery (LAD) with hemodynamically insignificant coronary artery disease. Cardiac computed tomography angiography was performed to identify the course and distribution of the RCA, which revealed a right dominant circulation with an anomalous RCA arising from the LAD, coursing between the aorta and pulmonary artery (Figure 1). The caliber of the vessel in this region appeared to be small but not significantly stenosed in comparison with a more normal distal caliber. Cardiothoracic surgery consultation was sought. Although single-vessel coronary artery bypass grafting was initially considered, the decision was later made to manage the patient conservatively. Alcohol cessation was strongly advised. Standard heart failure medications, including β-blockers and angiotensin-converting enzyme inhibitors, were prescribed. There was no improvement in left ventricular ejection fraction on the follow-up echocardiogram. Implantable cardioverter defibrillator placement was recommended but the patient refused. The patient has been stable without any cardiac events on follow-up visits.
Discussion
Anomalous coronary arteries have varied clinical outcomes, depending on the anomaly found. The symptoms range from a totally asymptomatic status to sudden cardiac death (SCD). This has been a subject of multiple clinical and autopsy studies to date. International studies show a relatively consistent incidence of anomalous coronaries of less than 1.5%1-6; these studies cite the right coronary anomaly as the most common, with the exception of one study2 in which the circumflex artery was noted to be the most common anomalous vessel. The incidence of an anomalous RCA is variable in different populations. The highest reported incidence has been in Indians (0.46%) and the lowest has been in Germans (0.04%).4-16 Origins of anomalous RCA are variable and may arise from the contralateral sinus, descending thoracic aorta, left main coronary, left circumflex artery, above or from the left sinus of Valsalva, the pulmonary arteries, or even below the aortic valve.1,3,4,15-21
RCA anomalies can involve origin and/or course of the artery. When the RCA arises anomalously from the left coronary sinus,1-6 it often follows a course between two great vessels and is particularly prone to compression. A single left coronary artery arising from the left coronary sinus is a rare anomaly, with the RCA arising from either the left main stem or the branches downstream from the main stem. Coming off the left main stem, the anomalously arising RCA can course anteriorly, posteriorly, or between the great arteries. The last course suggests a malignant type of anomaly due to the risk of extrinsic compression. An RCA arising from the LAD in the absence of a normally situated right coronary ostium is considered a variant of a single left coronary artery. Only 10 such cases have been described in the literature to date.7-13 In most of these cases, the RCA arises from the proximal or mid LAD and courses to the right toward the right atrioventricular groove or the margin of the right ventricle, with resulting ischemic symptoms primarily due to stenotic disease in the LAD or, rarely, in the RCA.7-11
Most anomalies are asymptomatic and are seen as incidental findings on coronary angiography Clinically symptomatic presentations include exertional angina, myocardial infarction, arrhythmias, and even SCD. The exact pathophysiologic basis of ischemia is unclear in cases of a single coronary artery without obstructive lesions arising from either the left or right sinus of Valsalva. It could be related to mechanical compression of an anomalous coronary artery between the aorta and pulmonary artery, particularly during exercise.1,21,22 Another proposed mechanism is the presence of valve-like ridges and the acute angulation of the artery as it traverses from left to right.23 Also, slit-like coronary orifice, acute angle of take-off of the anomalous artery from the aorta, and the presence and length of intramural segments of coronary vessel with proximal intussusception of the ectopic artery within the aortic root24 are other possible causes. However, anomalous coronary arteries originating from the contralateral aortic sinus coursing between the pulmonary artery and the aorta have received much attention because of their association with SCD.25-28 Many patients with that type of abnormality are asymptomatic before the fatal event. Thus, when these patients are identified, aggressive surgical management is often recommended. Nonetheless, decisions regarding the management of asymptomatic patients with these coronary anomalies are less well defined. Amid significant controversy regarding the treatment strategy, mainly due to a paucity of data, some authors have suggested surgical management for younger patients with anomalous coronaries arising in the opposite sinus, whether they are symptomatic or not.29,30 The unpredictable nature of the clinical course, leading to ischemia and SCD among younger individuals with this kind of anomaly, is the primary reason for this recommendation. Various surgical options are available, including coronary bypass (with or without ligation of the anomalous vessel using an internal mammary [IM] or saphenous vein graft), coronary reimplantation, or unroofing procedures.31
Because the anomalous vessel may have a dynamic limitation of flow during exercise and decent flow at rest, there is a risk of graft closure due to competitive flow through the native vessel if it is bypassed. Although survival after bypass may be better when an IM graft is used, it is prone to atrophy due to competitive flow within the native vessel. Using an IM graft in younger patients may also limit the available revascularization options, should they require a repeat bypass at a future date.
Noticeable differences are seen in the presentation and clinical course among patients with anomalous left coronary artery (ALCA) and anomalous right coronary artery (ARCA) abnormalities. The majority of deaths have occurred in ALCA patients, whether previously diagnosed or not.32 This may justify surgical repair upon diagnosis in all ALCA patients. However, operative decisions regarding asymptomatic patients with ARCA must be evaluated subject to a risk-benefit analysis comparing the rate of occurrence of SCD and the number of asymptomatic patients who have the anomaly.33 Considerations for operative risks related to ARCA surgery, as well as surgical outcomes, are important in the decision-making process.
The clinical outcome of ARCA is often benign. The incidence of SCD in asymptomatic patients with ARCA is extremely low. Over the past 25 years, clinical reports describe 10 patients with an RCA arising from the left coronary artery sinus who died suddenly. Eckart and colleagues34 screened 6.3 million military recruits for SCD over a 25-year period for the Department of Defense Medical Mortality Registry. Basso and colleagues27 reviewed two large registries in the United States and Italy, reporting SCD in young competitive athletes over a 10- to 20-year period; 27 deaths were recorded in patients who had no history of symptoms, 14 patients had an LCA arising from the right coronary sinus, and only 1 patient had an RCA arising from the left coronary sinus.
Brothers and associates35 reported significant subclinical changes indicative of myocardial ischemia in postoperative patients after surgical unroofing procedures. In their report, 9 of the 24 patients met criteria for ischemia at a mean of 15 months after surgical repair. These included 8 of 16 patients with ARCA and only 1 of 10 with ALCA. Thus, based on this postsurgical report, a more conservative approach is probably ideal in asymptomatic patients with an ARCA. ![]()
References
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28-40.
- Click RL, Holmes DR Jr, Vlietstra RE, et al. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival-a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13:531-537.
- Ayalp R, Mavi A, Sercelik A, et al. Frequency in the anomalous origin of the right coronary artery with angiography in a Turkish population. Int J Cardiol. 2002;82:253-257.
- Garg N, Tewari S, Kapoor A, et al. Primary congenital anomalies of the coronary arteries: a coronary: arteriographic study. Int J Cardiol. 2000;74:39-46.
- Topaz O, DeMarchena EJ, Perin E, et al. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol. 1992;34:129-138.
- Zhang F, Ge JB, Qian JY, et al. Frequency of the anomalous coronary origin in the Chinese population with coronary artery stenosis [in Chinese]. Zhonghua Nei Ke Za Zhi. 2005;44:347-349.
- Chatterjee T, Erne P. Anomalous right coronary artery originating from the mid left main coronary artery. Heart. 2003;89:132.
- Iyisoy A, Kursaklioglu H, Barcin C, et al. Single coronary artery with anomalous origin of the right coronary artery as a branch from the left anterior descending artery: a very rare coronary anomaly. Heart Vessels. 2002;16:161-163.
- Moretti C, De Felice F, Mazza A, Borello G. Anomalous origin of the right coronary artery from the left anterior descending coronary artery: a case report. G Ital Cardiol. 1999;29:915-917.
- Rath S, Battler A. Anomalous origin of the right coronary artery from the left anterior descending coronary artery. Cathet Cardiovasc Diagn. 1998;44:328-329.
- Biffani G, Lioy E, Loschiavo P, Parma A. Single coronary artery, anomalous origin of the right coronary artery from the left anterior descending artery. Eur Heart J. 1991;12:1326-1329.
- Amasyali B, Kursaklioglu H, Kose S, et al. Single coronary artery with anomalous origin of the right coronary artery from the left anterior descending artery with a unique proximal course. Jpn Heart J. 2004;45:521-525.
- Hamodraka ES, Paravolidakis K, Apostolou T. Posterior descending artery as a continuity from the left anterior descending artery. J Invasive Cardiol. 2005;17:343.
- Kamran M, Bogal M. Anomalous right coronary artery originating from the left anterior descending artery. J Invasive Cardiol. 2006;18:E221-E222.
- Cieslinski G, Rapprich B, Kober G. Coronary anomalies: incidence and importance. Clin Cardiol. 1993;16:711-715.
- Husaini SN, Beaver WL, Wilson IJ, Lach RD. Anomalous right coronary artery arising from left mainstem. Cathet Cardiovasc Diagn. 1983;9:407-409.
- Ayala F, Badui E, Murillo H, et al. Right coronary ostium agenesis with anomalous origin of the right coronary artery from an ectasic circumflex artery. A case report. Angiology. 1995;46:637-639.
- Cheatham JP, Ruyle NA, McManus BM, Gammel GE. Origin of the right coronary artery from the descending thoracic aorta: angiographic diagnosis and unique coronary artery anatomy at autopsy. Cathet Cardiovasc Diagn. 1987;13:321-324.
- Lauer B, Thiele H, Schuler G. A “new” coronary anomaly: origin of the right coronary artery below the aortic valve. Heart. 2001;85:486.
- Ho JS, Strickman NE. Anomalous origin of the right coronary artery from the left coronary sinus: case report and literature review. Tex Heart Inst J. 2002;29: 37-39.
- Kardos A, Babai L, Rudas L, et al. Epidemiology of congenital coronary artery anomalies: a coronary arteriography study on a central European population. Cathet Cardiovasc Diagn. 1997;42:270-275.
- Lipton MJ, Barry WH, Obrez I, et al. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39-47.
- Lopushinsky SR, Mullen JC, Bentley MJ. Anomalous right coronary artery originating from the left main coronary artery. Ann Thorac Surg. 2001;71: 357-358.
- Angelini P. Coronary artery anomalies: an entity in search of an identity. Circulation. 2007;115:1296-1305.
- Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, a not-so-minor congenital anomaly. Circulation. 1974;50:780-787.
- Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalous right or left coronary artery from the contralateral coronary sinus: “high-risk” abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. Am Heart J. 1997;133:428-435.
- Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000;35:1493-1501.
- Davis JA, Cecchin F, Jones TK, Portman MA. Major coronary artery anomalies in a pediatric population: incidence and clinical importance. J Am Coll Cardiol. 2001;37:593-597.
- Cohen AJ, Grishkin BA, Helsel RA, Head HD. Surgical therapy in the management of coronary anomalies: emphasis on utility of internal mammary artery grafts. Ann Thorac Surg. 1989;47:630-637.
- Pelliccia A. Congenital coronary artery anomalies in young patients: new perspectives for timely identification. J Am Coll Cardiol. 2001;37:598-600.
- Krasuski RA, Magyar D, Hart S, et al. Long-term outcome and impact of surgery on adults with coronary arteries originating from the opposite coronary cusp. Circulation. 2011;123:154-162.
- Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol. 1992;20:640-647.
- Gersony WM. Management of anomalous coronary artery from the contralateral coronary sinus. J Am Coll Cardiol. 2007;50:2083-2084.
- Eckart RE, Scoville SL, Campbell CL, et al. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med. 2004;141:829-834.
- Brothers JA, McBride MG, Seliem MA, et al. Evaluation of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery in a series of pediatric patients. J Am Coll Cardiol. 2007;50:2078-2082.