Laboratory-induced Mental Stress, Cardiovascular Response, and Psychological Characteristics
Li-Mei Liao RN, PhD,1 Mary G. Carey, RN, PhD2
1West China Hospital, Chengdu, Sichuan, China; 2Strong Memorial Hospital, Rochester, NY
Vulnerable populations, such as firefighters and patients with coronary artery disease, are susceptible to mental stress-induced cardiac events, including death. Mental stress tests are widely applied to investigate the mechanisms linking psychological stress to cardiovascular consequences and to predict the risk of death in those susceptible populations. However, some aspects of mental stress tests have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool. This review identifies types of mental stress tests applied in recent research and the exact cardiovascular responses induced by each mental stress test, along with the consideration of the influence of psychological characteristics on cardiovascular reactivity.
[Rev Cardiovasc Med. 2015;16(1):28-35 doi: 10.3909/ricm0730]
© 2015 MedReviews®, LLC
Laboratory-induced Mental Stress, Cardiovascular Response, and Psychological Characteristics
Li-Mei Liao RN, PhD,1 Mary G. Carey, RN, PhD2
1West China Hospital, Chengdu, Sichuan, China; 2Strong Memorial Hospital, Rochester, NY
Vulnerable populations, such as firefighters and patients with coronary artery disease, are susceptible to mental stress-induced cardiac events, including death. Mental stress tests are widely applied to investigate the mechanisms linking psychological stress to cardiovascular consequences and to predict the risk of death in those susceptible populations. However, some aspects of mental stress tests have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool. This review identifies types of mental stress tests applied in recent research and the exact cardiovascular responses induced by each mental stress test, along with the consideration of the influence of psychological characteristics on cardiovascular reactivity.
[Rev Cardiovasc Med. 2015;16(1):28-35 doi: 10.3909/ricm0730]
© 2015 MedReviews®, LLC
Laboratory-induced Mental Stress, Cardiovascular Response, and Psychological Characteristics
Li-Mei Liao RN, PhD,1 Mary G. Carey, RN, PhD2
1West China Hospital, Chengdu, Sichuan, China; 2Strong Memorial Hospital, Rochester, NY
Vulnerable populations, such as firefighters and patients with coronary artery disease, are susceptible to mental stress-induced cardiac events, including death. Mental stress tests are widely applied to investigate the mechanisms linking psychological stress to cardiovascular consequences and to predict the risk of death in those susceptible populations. However, some aspects of mental stress tests have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool. This review identifies types of mental stress tests applied in recent research and the exact cardiovascular responses induced by each mental stress test, along with the consideration of the influence of psychological characteristics on cardiovascular reactivity.
[Rev Cardiovasc Med. 2015;16(1):28-35 doi: 10.3909/ricm0730]
© 2015 MedReviews®, LLC
KEY WORDS
Mental stress • Cardiovascular response • Psychological characteristics
KEY WORDS
Mental stress • Cardiovascular response • Psychological characteristics
… mental stress tests have been used as a prognostic tool to predict the risk of subsequent cardiac death in patients with CAD.
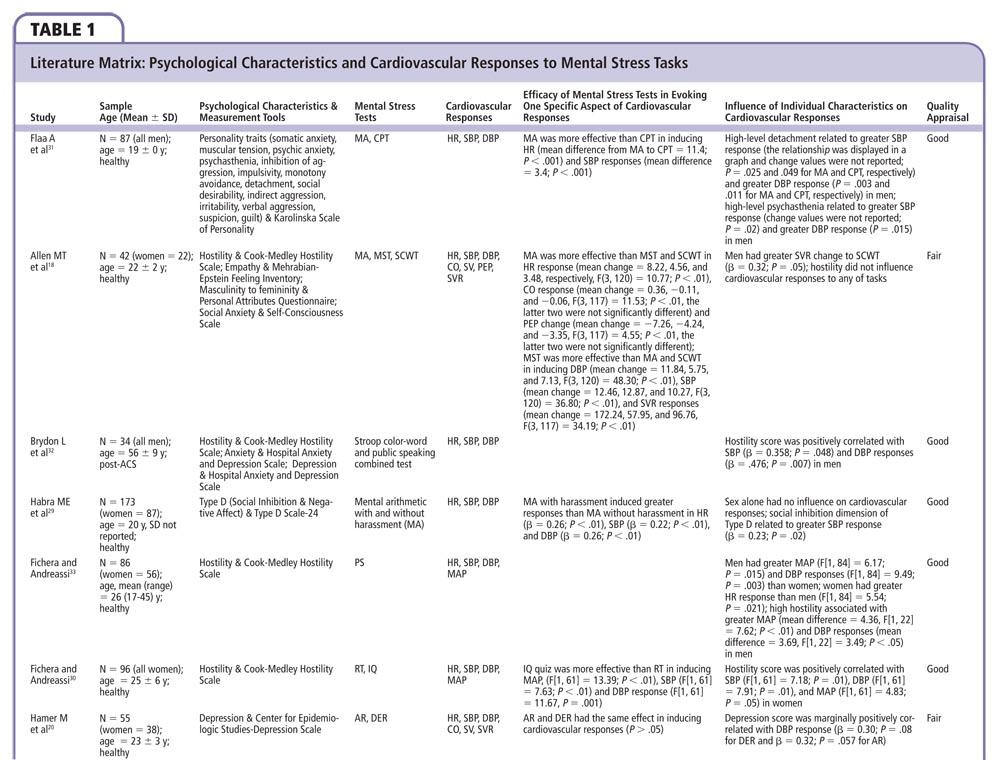
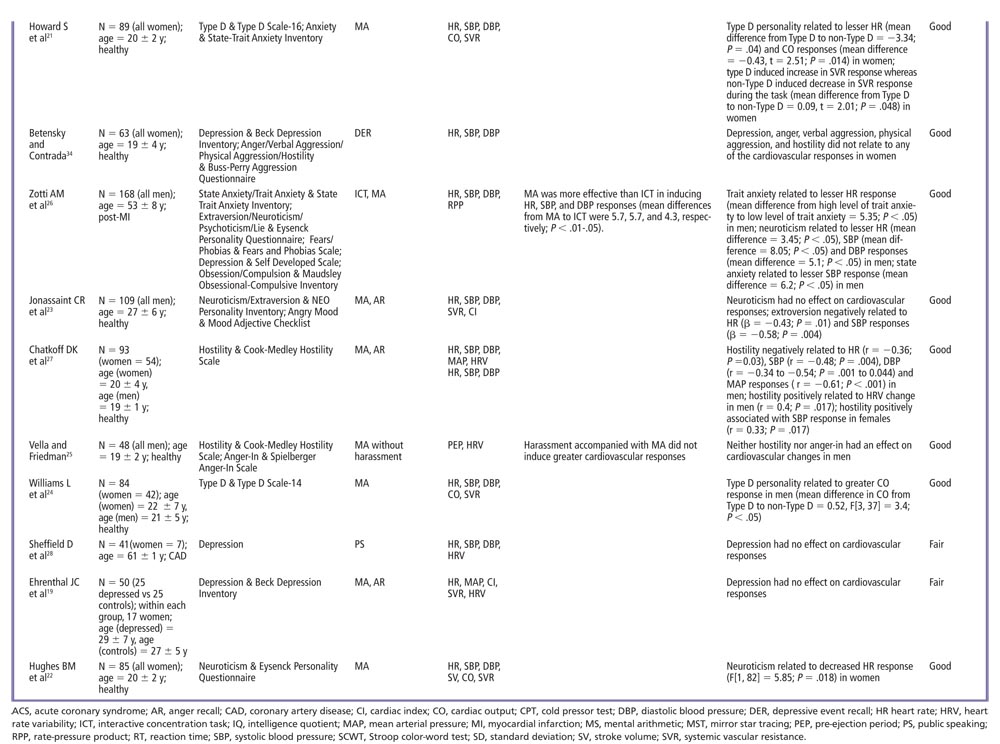
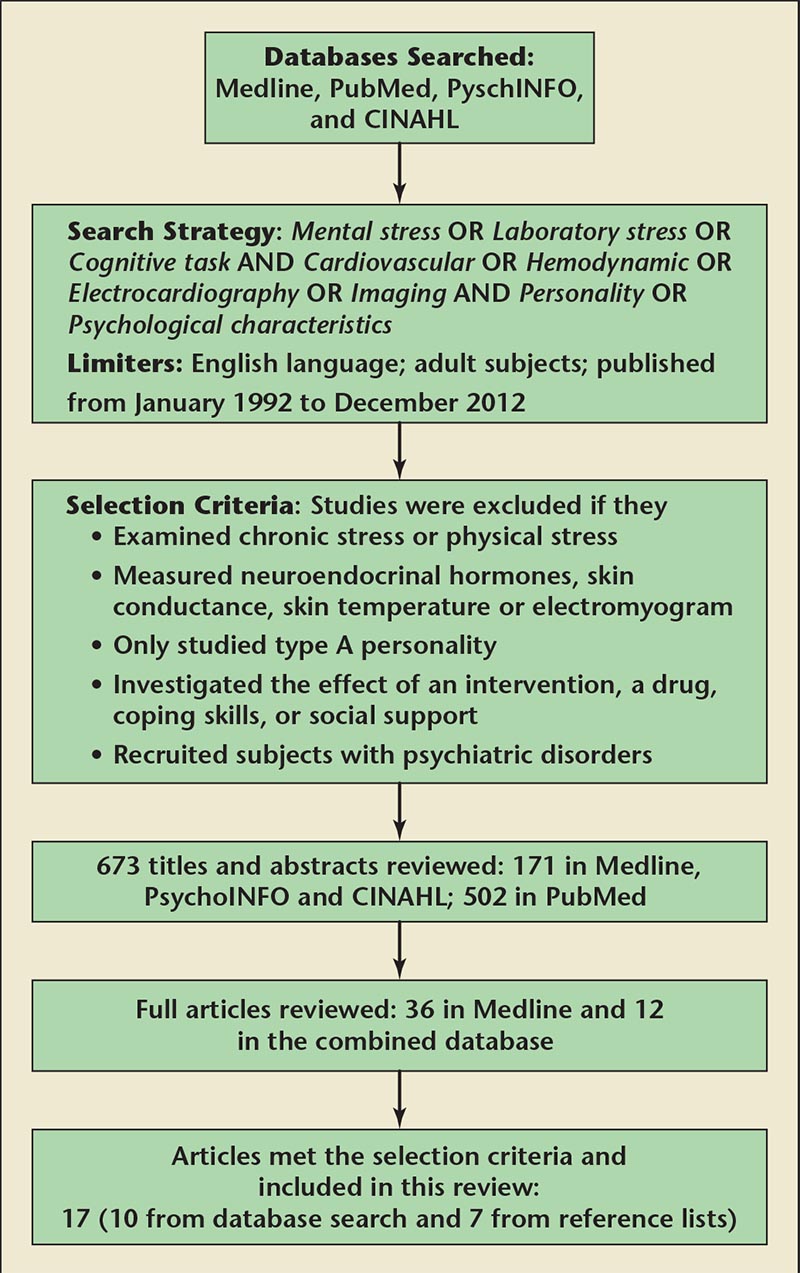
Figure 1. Flow chart of systematic review. CINAHL, Cumulative Index to Nursing and Allied Health Literature.
This review revealed that neither depression nor anger had effect on cardiovascular reactivity to mental stress tests.
… mental arithmetic is more effective than other tests in inducing most cardiovascular responses, with the exception of systemic vascular resistance.
Main Points
• Vulnerable populations, such as firefighters and patients with coronary artery disease, are susceptible to mental stress-induced cardiac events, including death. Mental stress tests are widely applied to investigate the mechanisms linking psychological stress to cardiovascular consequences and to predict the risk of death in susceptible populations.
• Some aspects of mental stress tests, however, have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool.
• Mental stress tests should be standardized with regard to procedure and contents. More studies recruiting cardiovascular patients are needed in order to clarify the exact cardiovascular responses in this population. Future studies should use an identical scale to measure similar psychological characteristics.
Main Points
• Vulnerable populations, such as firefighters and patients with coronary artery disease, are susceptible to mental stress-induced cardiac events, including death. Mental stress tests are widely applied to investigate the mechanisms linking psychological stress to cardiovascular consequences and to predict the risk of death in susceptible populations.
• Some aspects of mental stress tests, however, have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool.
• Mental stress tests should be standardized with regard to procedure and contents. More studies recruiting cardiovascular patients are needed in order to clarify the exact cardiovascular responses in this population. Future studies should use an identical scale to measure similar psychological characteristics.
In the cardiovascular field, mental stress is implicitly perceived by most researchers as mental arousal with or without emotional reaction.1,2 Mental stress exists in daily life and evokes physiologic reactions.3-5 In vulnerable populations, such as firefighters who work under stressful conditions and patients with cardiovascular disease, mental stress can result in severe consequences such as myocardial ischemia and cardiac death. Cardiac death among firefighters was 3 to 14 times more likely to happen during an alarm response than during nonemergency duty.6 The number of deaths from coronary artery disease (CAD) on the day of the Northridge, CA, earthquake in 1994 was six times higher than the same days in previous years.7
In order to investigate the effect of mental stress on cardiac activity, laboratory mental stress tests have been introduced to the cardiovascular field that adopt a battery of laboratory stimuli, such as public speaking, color-word conflict, and mental arithmetic deduction, to evoke cardiovascular responses. In the past 20 years, many researchers have applied mental stress tests to explore mechanisms in the development of CAD and the occurrence of cardiac events. Some mechanisms related to hemodynamic alteration, endothelial dysfunction, and circulating inflammatory factors have been proposed as possible mechanisms linking psychological stress to cardiovascular consequences.3,4 In addition, mental stress tests have been used as a prognostic tool to predict the risk of subsequent cardiac death in patients with CAD. The results showed that the predictive value of mental stress tests was better than that of exercise stress tests.8
Although mental stress tests have been applied widely in medical and psychological research and seem to be a better and inexpensive predictive tool for the subsequent cardiac events in susceptible populations, some aspects of mental stress tests have not been thoroughly understood, which impairs their reliability and validity as a research and clinical tool. First, how do the numerous confounding factors, especially psychological ones, moderate the relationship between mental stress and cardiovascular responses? Second, how do a variety of stressors performed in mental stress tests affect cardiovascular responses, and what is the order of their efficacy in inducing cardiovascular responses? This review summarizes current evidence of the role psychological characteristics play on the cardiovascular reactivity to mental stress tests and which mental stress tests are considered to be most effective in inducing such responses.
Methods
Search Strategy
To identify relevant articles, electronic searches were performed in PubMed, Medline, Psychlnfo, and the Cumulative Index to Nursing & Allied Health Literature combined database from November 2012 to December 2012. The main search terms were Mental stress OR Laboratory stress OR Cognitive task AND Cardiovascular OR Hemodynamic OR Electrocardiography OR Imaging AND Personality OR Psychological characteristics. The search was limited to articles with experimental study design comparing the efficacy of at least two mental stress tests or the effect of psychological factors on cardiovascular reactivity, written in English and using adult human subjects. In addition, reference lists of retrieved articles were manually screened. The initial search found that most studies on psychological characteristics and cardiovascular responses to mental stress tests were conducted in the past 20 years. Therefore, the search was limited to the articles published from January 1992 to December 2012.
Selection Criteria
The mental stress test was defined as a test with stressor(s) conducted in a laboratory setting. Cardiovascular responses were defined as the alterations in hemodynamics (heart rate, blood pressure, and systemic vascular resistance), electrocardiogram (ECG; ST-segment elevation and depression, heart rate variability, T-wave alternans), and cardiac images (wall motion abnormality, cardiac output, left ventricular ejection fraction). Studies measuring neuroendocrine hormones (salivary and blood cortisol), skin conductance, skin temperature, and electromyogram were excluded. Chronic stress (job and caregiver stress), social stress (marital and school stress), and physical stress (bike and treadmill stress test) were excluded. Studies focusing on the effect of an intervention, a drug, coping skills, or social support were excluded. Studies specifically investigating type A personality were excluded because type A personality has not been considered to be a valid psychological characteristic related to CAD on the basis of the negative findings of large-scale studies and meta-analyses.9-11 Type D personality (a detachment and negative affect personality) is the alternative to type A, which was identified by Denollet and colleagues12 when they investigated the coping styles in men with coronary heart disease. The association between type D personality and progression of CAD and cardiac death was repeatedly reported by researchers.13-16 Therefore, type D personality was considered one of the interested psychological characteristics in the review; articles studying type D personality were included. In addition, studies recruiting psychiatric patients were excluded.
Quality Appraisal
The quality of the included studies was assessed to investigate internal validity based on the following criteria17: (1) Is the comparison group comparable (eg, is the influence of sex and other confounders excluded)? (2) Are the researchers blinded to the classification of the sample on the basis of psychological characteristics? (3) Is the sample size adequate for the analytic methods? (4) Are psychological characteristics adequately measured? (5) Are tools for measurement of cardiovascular responses reliable? The selected studies were classified into good-quality or fair-quality groups on the basis of compliance with at least three quality criteria.
Data Extraction
For each selected article, data were extracted including first author, publication year, sample size with demographic and clinical characteristics, mental stress tests, psychological characteristics and measurement scales, cardiovascular response indicators, and the influence of psychological characteristics on cardiovascular responses.
Findings
A total of 673 articles were reviewed initially. Ten articles met the selection criteria and were included in this analysis. Seven more studies were found from the reference lists of retrieved articles (one was published in 1991 and was included also because of its relevance). A total of 17 articles are included in the final analysis (Figure 1) with extracted data reported in Table 1.
Sample Size, Demographic, and Clinical Characteristics
The sample size of the included studies ranged from 34 to 173 subjects (83 ± 40 subjects). Three studies (18%) had a small sample size with < 50 subjects and 3 studies (18%) had a large sample size with > 100 subjects. The majority of the included studies (n = 13; 77%) recruited healthy young adults. Their mean age was < 30 years. Among them, nearly half of the studies (n = 6) recruited college students with a mean age of < 20 years. Eight studies (47%) included both men and women. Five studies (29%) included only men, and four studies (24%) recruited only women. Three studies (19%) recruited patients with coronary heart disease and one study recruited depressive patients.
Indicators of Cardiovascular Responses
All of the enrolled studies adopted heart rate, systolic blood pressure, and diastolic blood pressure as the indicators of cardiovascular responses. Other measured hemodynamic outcomes were systemic vascular resistance and cardiac output,18-24 stroke volume,20,22 pre-ejection time,18,25 and rate-pressure product.26 All the hemodynamic values were obtained using noninvasive approaches, such as an impedance cardiograph instrument or the Finomer device (FMS, Finapres Measurement Systems, Arnhem, The Netherlands). Five studies (29%) assessed heart rate variability—an ECG parameter. No study measured imaging changes of the heart to mental stress strategies.19,22,25,27,28
Mental Stress Tests and Their Efficacy in Inducing Cardiovascular Responses
Ten mental stress tests were employed in the reviewed studies, including mental arithmetic, Stroop color-word test, public speaking, anger recall, depressive event recall, cold pressor test, mirror star tracing, reaction time, intelligence quotient quiz, and interactive concentration task. Mental arithmetic was most frequently used. It was adopted in 11 selected studies (65%) and was followed by anger/depressive event recall in eight studies (47%). Public speaking and color-word conflict each were used in two studies (12%). One study used a combined test of color-word test plus public speaking. Each mental stress test is described in the literature, but briefly, a mental arithmetic test asks the subject to sequentially subtract a number from a given large number; in a Stroop color-word test, a word is displayed in a color different from the color it actually names and the subject is required to speak out the color of the word; a public speaking test asks the subject to give a speech about a real-life situation such as a loved one receiving poor care in a hospital in front of an audience; in anger/depressive event recall, the subject recalls and reports a life event which evokes anger/depression; a cold pressor test is performed by asking the subject to put a hand into ice water for as long as tolerable; a mirror star tracing requires the subject to move a pencil to trace the diagram of a star while looking at the hand only reflected in a mirror; in a reaction time test, the subject presses a button rapidly in response to specific stimuli, such as a sound; and an intelligent quotient quiz requires the subject to answer difficult questions related to geography, math, history, and vocabulary in a limited period of time. Interactive concentration tasks consist of problem solving, concentration, and rapid psychomotor performance.
Mental arithmetic was performed in different ways in the selected studies. Five studies (29%) applied identical subtraction problems to all subjects. In the other two studies, subtraction problems were varied in level of difficulty and were selected based on the subject's math capacity. One study18 incorporated a motion component into the mental arithmetic (participants selected the letter corresponding to their answer on a slide and pressed the appropriate button on a control panel as quickly as possible), whereas another two studies25,29 added competition (a bonus for the best performer) and disturbance components (verbal harassment delivered to the participant).
Seven studies8,20,25,26,29-31compared the efficacy of mental stress tests in inducing cardiovascular responses. Mental arithmetic was more effective than mirror star tracing, Stroop color-word conflict, cold pressor, and interactive concentration tests in provoking most cardiovascular responses except systematic vascular resistance. Mirror star tracing was more effective in provoking a systemic vascular resistance reaction.18 Results regarding the effect of harassment were inconsistent.25,29
Psychological Characteristics and Their Effects on Cardiovascular Responses
The enrolled studies examined a variety of psychological characteristics, including anxiety, aggression, psychasthenia, impulsivity, monotony avoidance, detachment, social desirability, irritability, suspicion, guilt, hostility, empathy, type D personality, masculinity, femininity, depression, anger, extroversion, neuroticism, psychoticism, fears and phobias, obsession, compulsion, hedonic arousal, tense arousal, and energetic arousal. The most frequently examined psychological characteristic was hostility, which was investigated in seven studies (41%). Other investigated psychological characteristics, in the order of frequency, were depression in six studies (35%), anxiety and anger, each in five studies (29%), and type D personality in three studies (18%).
All the studies used self-report scales to measure psychological characteristics. Hostility was measured with the Cook-Medley Hostility Scale25, 27,30,32,33 and Buss-Perry Aggression Questionnaire.34 Depression was assessed with five different tools: the Beck Depression Inventory,19,34 the Center for Epidemiologic Studies Depression Scale (CESD),20 the Hospital Anxiety and Depression Scale,32 the Minnesota Multiphasic Personality Inventory-Depression Scale,28 and a scale developed by the investigators.26 Anxiety was measured with the state-trait anxiety inventory.21,22 Type D personality was assessed using the Type D scale with 14, 16, or 24 items.21,24,29
This review revealed that neither depression nor anger had an effect on cardiovascular reactivity to mental stress tests. With regard to hostility, results from the included studies were inconsistent. Three studies30,32,33 showed that individuals with a high level of hostility had greater reactivity in blood pressure, whereas another three studies18,25,34 did not find any moderating effect. Results from Chatkoff and colleagues27 were different. They reported that a high level of hostility increased systolic blood pressure reactivity but decreased diastolic blood pressure response. For anxiety, Zotti and associates26 reported that a high level of anxiety was associated with fewer cardiovascular responses. Analysis of the results of the included studies revealed that type D personality had different moderating effects on different cardiovascular response indicators; that is, type D personality decreased heart rate response but increased blood pressure and systemic vascular resistance responses.21,29,31 Subgroup analysis regarding the dimensions of type D personality suggested that the effect on blood pressure mainly originated from the social inhibition dimension (detachment was the synonym of social inhibition in the study by Flaa and associates).29,31
Discussion
This review reveals that mental arithmetic is more effective than other tests in inducing most cardiovascular responses, with the exception of systemic vascular resistance. Sympathetic β-adrenergic activity elicited by mental arithmetic may explain the more potent effect on the heart than on the vessels, but it cannot explain why mental arithmetic is more effective than other tests.35 Research on this mechanism is needed.
The effects of psychological characteristics on cardiovascular responses are inconclusive. All the results on depression in this review were consistently negative. However, due to the sample size of the included studies, the results are very likely to be false. The results regarding anger, anxiety, and type D personality were extracted from only one to three articles. No reliable conclusion can be made on the basis of these limited data. There is also variation in the results among the seven studies that studied the effect of hostility on cardiovascular responses. To ensure that this variation is not stemming from the quality of the studies included and participant population, a χ2 test was performed, which did not show a significant difference. Researchers have proposed many theories on how hostility translates into cardiovascular alterations (eg, excessive nervous activation in hostile people resulted in downregulation of β-adrenergic receptors, which was associated with blunted vasodilation and a subsequent increase in systemic vascular resistance and elevated blood pressure).36,37 However, more studies clarifying the association are needed before this mechanism can be explored further.
Based on this review, we have several recommendations with regard to the development of a mental stress test that is a reliable tool for research and clinical application. First, mental stress tests should be standardized with regard to procedure and content. Second, more studies recruiting cardiovascular patients are needed in order to clarify the exact cardiovascular responses in this population. Third, future studies should utilize an identical scale to measure similar psychological characteristics (currently, different scales are being used). The underlying definitions and dimensions the scales measure may be different; for example, both the Beck Depression Inventory and the CESD are intended to assess depression. However, the Beck Depression Inventory concentrates on somatic symptoms, whereas the CESD focuses on cognitive and affective symptoms.38 They are correlated but do not evaluate the same construct of depression. Finally, selection of a mental stress test for research or clinical application should depend on the efficacy of a test and the research or clinical purpose (eg, mental arithmetic is more effective in evoking the heart response, whereas mirror star tracing is more effective in evoking the vessel response). If the purpose is to screen hypertension, mirror star tracing may be more suitable. The meta-analysis by Chida and Hamer39 reviewed the effect of all mental stress tests as the same and conceals this important information.
Conclusions
The associations between mental stress tests, psychological charac teristics, and cardiovascular responses are wide-ranging and complex. The mental stress tests are not reliable enough as a research and clinical tool on the basis of current evidence. More studies are needed to clarify questions related to mental stress tests. ![]()
The authors report no real or apparent conflicts of interest.
References
- Gullette EC, Blumenthal JA, Babyak M, et al. Effects of mental stress on myocardial ischemia during daily life. JAMA. 1997;277:1521-1526.
- Gabbay FH, Krantz DS, Kop WJ, et al. Triggers of myocardial ischemia during daily life in patients with coronary artery disease: physical and mental activities, anger and smoking. J Am Coll Cardiol. 1996;27: 585-592.
- Goldberg AD, Becker LC, Bonsall R, et al. Ischemic, hemodynamic, and neurohormonal responses to mental and exercise stress. Experience from the Psychophysiological Investigations of Myocardial Ischemia Study (PIMI). Circulation. 1996;94:2402-2409.
- Ghiadoni L, Donald AE, Cropley M, et al. Mental stress induces transient endothelial dysfunction in humans. Circulation. 2000;102:2473-2478.
- Lampert R, Jain D, Burg MM, et al. Destabilizing effects of mental stress on ventricular arrhythmias in patients with implantable cardioverter-defibrillators. Circulation. 2000;101:158-164.
- Kales SN, Soteriades ES, Christophi CA, Christiani DC. Emergency duties and deaths from heart disease among firefighters in the United States. N Engl J Med. 2007;356:1207-1215.
- Leor J, Poole WK, Kloner RA.. Sudden cardiac death triggered by an earthquake. N Engl J Med. 1996;334:413-419.
- Sheps DS, McMahon RP, Becker L, et al. Mental stress-induced ischemia and all-cause mortality in patients with coronary artery disease: results from the Psychophysiological Investigations of Myocardial Ischemia study. Circulation. 2002;105:1780-1784.
- Myrtek M. Meta-analyses of prospective studies on coronary heart disease, type A personality, and hostility. Int J Cardiol. 2001;79:245-251.
- Gallacher JE, Sweetnam PM, Yarnell JW, et al. Is type A behavior really a trigger for coronary heart disease events? Psychosom Med. 2003;65:339-346.
- Myrtek M. Type A behavior pattern, personality factors, disease, and physiological reactivity: a meta-analytic update. Pers Individ Diff. 1995;18: 491-502.
- Denollet J, Sys SU, Brutsaert DL. Personality and mortality after myocardial infarction. Psychosom Med. 1995;57:582-591.
- Svansdottir E, Denollet J, Thorsson B, et al. Association of type D personality with unhealthy lifestyle, and estimated risk of coronary events in the general Icelandic population. Eur J Prev Cardiol. 2013;20:322-330.
- Grande G, Romppel M, Barth J. Association between type D personality and prognosis in patients with cardiovascular diseases: a systematic review and metaanalysis. Ann Behav Med. 2012;43:299-310.
- Denollet J, Sys SU, Stroobant N, et al. Personality as independent predictor of long-term mortality in patients with coronary heart disease. Lancet. 1996;347:417-421.
- Denollet J, Vaes J, Brutsaert DL. Inadequate response to treatment in coronary heart disease: adverse effects of type D personality and younger age on 5-year prognosis and quality of life. Circulation. 2000;102: 630-635.
- Jüni P, Altman DG, Egger M. Systematic reviews in health care: Assessing the quality of controlled clinical trials. BMJ. 2001;323:42-46.
- Allen MT, Stoney CM, Owens JF, Matthews KA. Hemodynamic adjustments to laboratory stress: the influence of gender and personality. Psychosom Med. 1993;55:505-517.
- Ehrenthal JC, Herrmann-Lingen C, Fey M, Schauenburg H. Altered cardiovascular adaptability in depressed patients without heart disease. World J Biol Psychiatry. 2010;11:586-593.
- Hamer M, Tanaka G, Okamura H, et al. The effects of depressive symptoms on cardiovascular and catecholamine responses to the induction of depressive mood. Biol Psychol. 2007;74:20-25.
- Howard S, Hughes BM, James JE. Type D personality and hemodynamic reactivity to laboratory stress in women. Int J Psychophysiol. 2011;80:96-102.
- Hughes BM, Howard S, James JE, Higgins NM. Individual differences in adaptation of cardiovascular responses to stress. Biol Psychol. 2011;86:129-136.
- Jonassaint CR, Why YP, Bishop GD, et al. The effects of neuroticism and extraversion on cardiovascular reactivity during a mental and an emotional stress task. Int J Psychophysiol. 2009;74:274-279.
- Williams L, O’Carroll RE, O’Connor RC. Type D personality and cardiac output in response to stress. Psychol Health. 2009;24:489-500.
- Vella EJ, Friedman BH. Hostility and anger in: cardiovascular reactivity and recovery to mental arithmetic stress. Int J Psychophysiol. 2009;72:253-259.
- Zotti AM, Bettinardi O, Soffiantino F, et al. Psychophysiological stress testing in postinfarction patients. Psychological correlates of cardiovascular arousal and abnormal cardiac responses. Circulation. 1991; 83(4 suppl):II25-II35.
- Chatkoff DK, Maier KJ, Javaid J, et al. Dispositional hostility and gender differentially relate to cognitive appraisal, engagement, and cardiovascular reactivity across cognitive and emotional laboratory tasks. Pers Individ Diff. 2009;47:122-126.
- Sheffield D, Krittayaphong R, Cascio WE, et al. Heart rate variability at rest and during mental stress in patients with coronary artery disease: differences in patients with high and low depression scores. Int J Behav Med. 1998;5:31-47.
- Habra ME, Linden W, Anderson JC, Weinberg J. Type D personality is related to cardiovascular and neuroendocrine reactivity to acute stress. J Psychosom Res. 2003;55:235-245.
- Fichera LV, Andreassi JL. Stress and personality as factors in women’s cardiovascular reactivity. Int J Psychophysiol. 1998;28:143-155.
- Flaa A, Ekeberg O, Kjeldsen SE, Rostrup M. Personality may influence reactivity to stress. Biopsychosoc Med. 2007;1:5.
- Brydon L, Strike PC, Bhattacharyya MR, et al. Hostility and physiological responses to laboratory stress in acute coronary syndrome patients. J Psychosom Res. 2010;68:109-116.
- Fichera LV, Andreassi JL. Cardiovascular reactivity during public speaking as a function of personality variables. Int J Psychophysiol. 2000;37:267-273.
- Betensky JD, Contrada RJ. Depressive symptoms, trait aggression, and cardiovascular reactivity to a laboratory stressor. Ann Behav Med. 2010;39:184-191.
- Obrist PA. Cardiovascular Psychophysiology: A Perspective. New York, NY: Plenum Press; 1981.
- Suarez EC, Sherwood A, Hinderliter AL. Hostility and adrenergic receptor responsiveness: evidence of reduced beta-receptor responsiveness in high hostile men. J Psychosom Res. 1998;44:261-267.
- Sherwood A, Hughes JW, Kuhn C, Hinderliter AL. Hostility is related to blunted beta-adrenergic receptor responsiveness among middle-aged women. Psychosom Med. 2004;66:507-513.
- Campbell SB, Cohn JF. Prevalence and correlates of postpartum depression in first-time mothers. J Abnorm Psychol. 1991;100:594-599.
- Chida Y, Hamer M. Chronic psychosocial factors and acute physiological responses to laboratory-induced stress in healthy populations: a quantitative review of 30 years of investigations. Psychol Bull. 2008;134:829-885.